2022–2023 Report on the Child and Youth Death Review and Analysis Unit
Read the committee’s review of child and youth deaths in Ontario in 2022 and 2023.
Acknowledgement
We would like to acknowledge and offer our sincerest condolences to all the families, friends, loved ones and communities that have been impacted by the tragic deaths of children and youth. We honour the sacredness of this work and acknowledge the privilege of learning from the journey of each unique child and youth.
We would also like to acknowledge and express our deep gratitude to all those who have provided input and feedback on our death review processes, helping us to continuously improve and do this important work in the best way possible.
Introduction
Office of the Chief Coroner
Ontario's death investigation system is the largest in North America. In Ontario, coroners are medical doctors with training in the principles of death investigation. Coroners investigate deaths in accordance with Section 10 of the Coroners Act. The Office of the Chief Coroner (OCC) investigates deaths involving non–natural causes, for example, injuries (both intentional and non–intentional) and those that occur suddenly and unexpectedly, to fully understand the circumstances of the deaths and to potentially provide recommendations to prevent further deaths. In addition, investigations are completed into deaths that occur in certain settings, for example, correctional facilities and under such circumstances where an investigation is believed to be required.
Death investigation services are provided by the OCC and the Ontario Forensic Pathology Service (OFPS). Together, they form a division within the Ministry of the Solicitor General (SOLGEN). The OCC partners with the OFPS to ensure a coordinated and collaborative approach to conducting death investigations in the public interest.
Definitions
The OCC applies the following definitions when determining the manner of death:
- Natural: Cause of death was a disease, or a complication of its treatment. Injury did not cause or substantially contribute to the death.
- Accident: Cause of death was an injury where death was not intended or foreseen. Inflicted injury did not cause or substantially contribute to the death.
- Suicide: Cause of death was an injury which was non–accidentally inflicted by the deceased.
- Homicide: Cause of death was an injury which was non–accidentally inflicted by a person other than the deceased.
- Undetermined: Cause of death could not be selected from the classifications of Natural, Accident, Suicide and Homicide because the evidence was either:
- inadequate, for example, skeletal remains
- equal for two or more classifications, or so nearly equal that they could not be confidently distinguished
- did not reasonably fit the definitions of any of the four classifications
Child and youth deaths in Ontario and Canada: Trends over time
While deaths of children and youth comprise a small percentage of all deaths investigated by the OCC, the OCC investigates approximately 44% of all child and youth deaths that occur within Ontario. The investigation and review of child and youth deaths is an area that continues to be one of the most important and challenging areas within the OCC’s mandate.
It is important to consider the findings published in this report within the broader context of deaths among children and youth in Canada.
Chart 1: Comparison of child and youth deaths in Canada, Ontario and Ontario coroner investigations (age 0–19, 2013–2023)
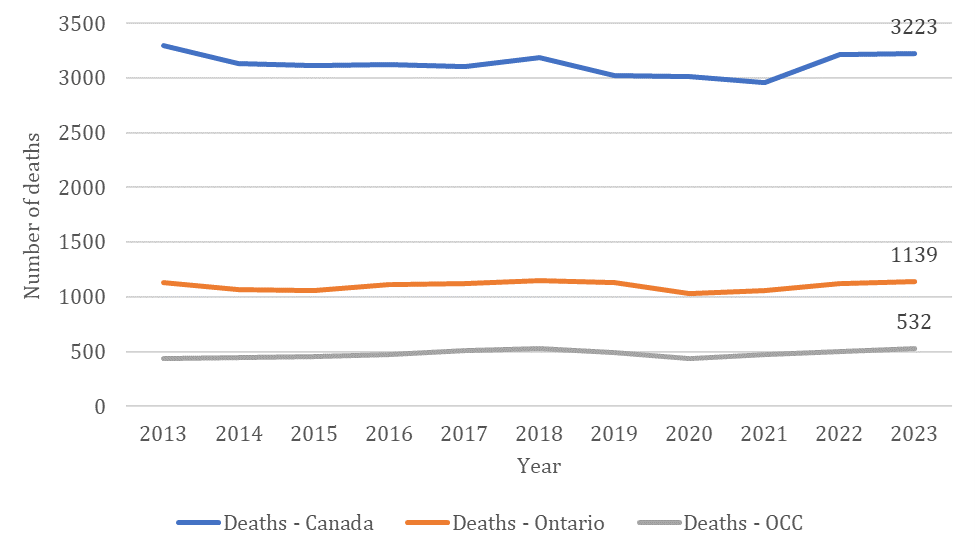
Chart 1 illustrates the number of annual child and youth deaths and compares the number of deaths investigated by the OCC with the provincial and national number of deaths. Between 2013 and 2023, the year–to–year totals have remained relatively consistent, except for a slightly increased number of deaths at a national level from 2021 to 2022.
| Year | Ontario | Canada | % of Ontario populations vs. Canada |
|---|---|---|---|
| 2013 | 3,078,716 | 7,858,925 | 39% |
| 2014 | 3,070,164 | 7,870,897 | 39% |
| 2015 | 3,062,245 | 7,886,794 | 39% |
| 2016 | 3,079,434 | 7,949,667 | 39% |
| 2017 | 3,095,381 | 8,002,681 | 39% |
| 2018 | 3,119,061 | 8,072,580 | 39% |
| 2019 | 3,131,045 | 8,122,020 | 39% |
| 2020 | 3,130,254 | 8,139,158 | 38% |
| 2021 | 3,094,198 | 8,078,797 | 38% |
| 2022 | 3,137,397 | 8,271,950 | 38% |
| 2023 | 3,197,499 | 8,424,747 | 38% |
| Year | Ontario | Canada | % of Ontario deaths vs. Canada |
|---|---|---|---|
| 2013 | 1,132 | 3,295 | 34% |
| 2014 | 1,066 | 3,135 | 34% |
| 2015 | 1,058 | 3,112 | 34% |
| 2016 | 1,116 | 3,120 | 36% |
| 2017 | 1,119 | 3,107 | 36% |
| 2018 | 1,147 | 3,179 | 36% |
| 2019 | 1,132 | 3,018 | 38% |
| 2020 | 1,013 | 2,971 | 34% |
| 2021 | 1,062 | 2957 | 36% |
| 2022 | 1,119 | 3213 | 35% |
| 2023 | 1,139 | 3,223 | 35% |
Chart 2 provides the number of child and youth deaths per year and shows the percentage of deaths in Ontario as a proportion of the national total. Between 2013 and 2023, the year–to–year totals have remained fairly consistent. In 2019, there was slight increase in the proportion of deaths in Ontario in comparison to the national total, however, it decreased again in the following years to 35% in 2023.
Chart 3: Distribution of child and youth deaths investigated by the OCC across age groups (2013–2023)
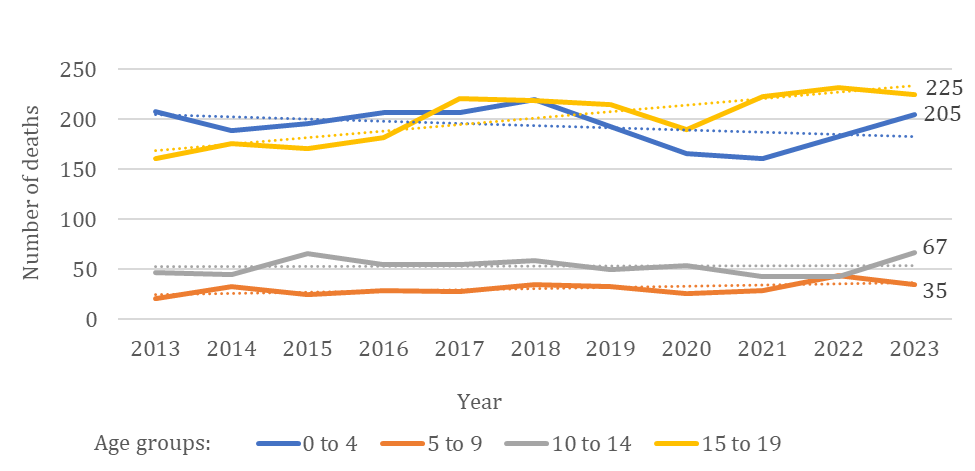
In 2022, the OCC investigated 502 deaths of children and youth, and 532 deaths in 2023. Although there was a small increase in the total number of deaths in 2023 compared with the previous year, Chart 3 shows the distribution of deaths among the age group in the two years was similar. In both years, the highest number of deaths investigated occurred among 15 to19 year olds, followed by infants aged 0–4 years.
Over a 10–year period, the number of deaths among the age group of 5 to 9 years, and 10 to 14 years have been consistently the lowest in comparison to the other age groups. There was a small decrease in the number of investigated deaths among infants and toddlers aged 0 to 4 years between 2019 and 2021, however the number increased for this age group in the most recent two years. Since 2017, the highest number of deaths investigated occurred among youth between the ages of 15 and 19 years of age in comparison to the rest of the age groups.
Chart 4: Manner of death in OCC investigations (ages 0–19, 2013–2023)
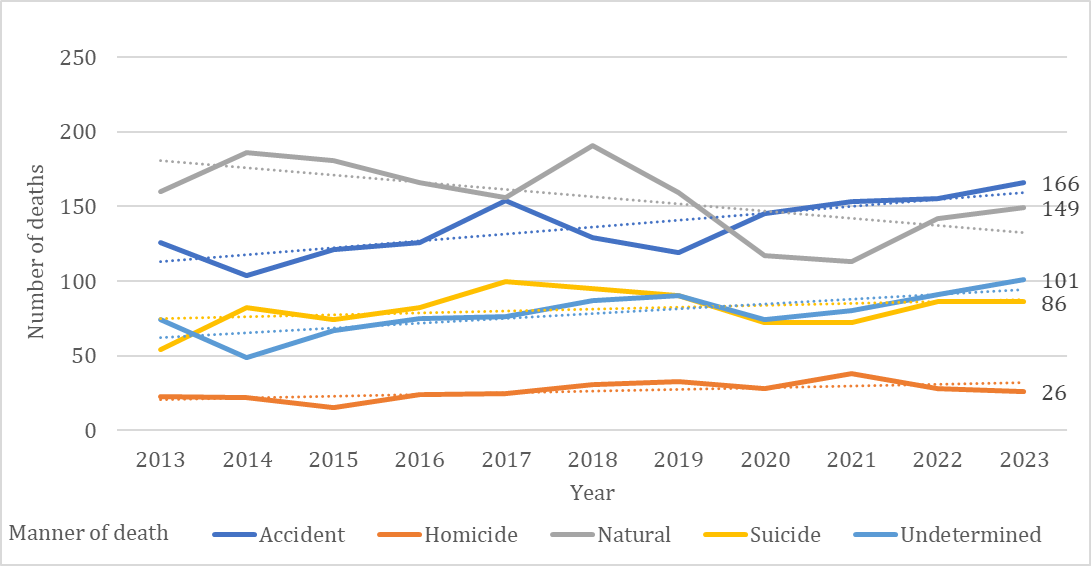
Note: approximately 8% of all the manner of deaths reported for 2023 are preliminary and may change in future reports. There were 4 deaths that were under investigation at the time of this report therefore did not have a manner of death.
Over a 10–year period, there was a small increase in the overall number of deaths with manners of homicide, suicide, and undetermined. Until 2020, natural deaths accounted for the highest number of deaths investigated among children and youth, however, from 2020 to 2023 accident was the most common manner of death.
Chart 5: Manner of death in OCC investigations – distribution across age groups in 2023
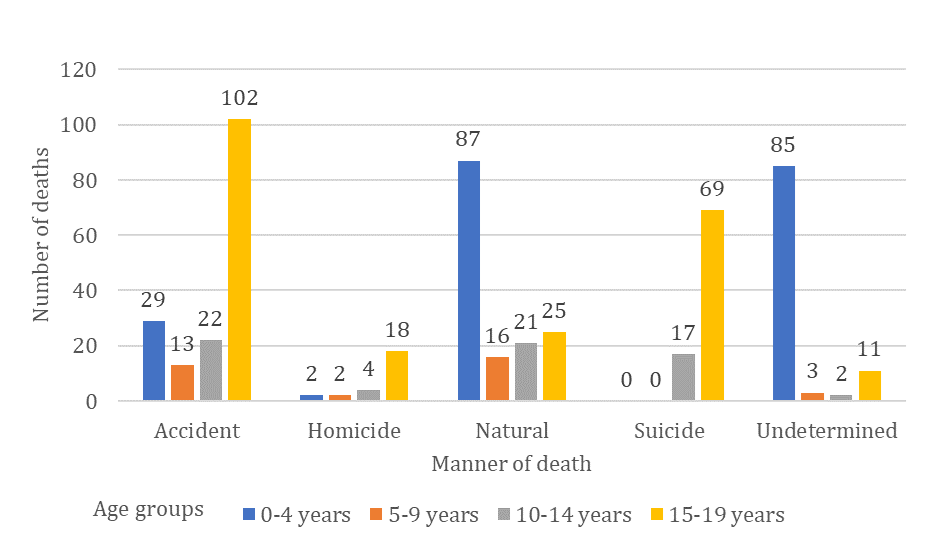
Chart 5 demonstrates the breakdown by each manner of death for each age group for deaths in 2023. Among the infants and toddlers of ages 0 to 4 years, natural deaths were most common, followed by undetermined manner of death. Accident was the most common manner of death among youth of ages 15 to 19 years, followed by suicide.
Accidental deaths among 0–19 year olds in 2023 (166 total)
- 37% died due to motor vehicle collision
- 19% died due to acute drug toxicity
- 18% died due to drowning
In 2023, the most common causes of accidental deaths across all ages were trauma from motor vehicle collision, acute drug toxicity, and drowning.
Death factors for accidental deaths among different age groups in 2023
Death factors — 0 to 4 years old
drowning (all types) — 41%
other — 42%
asphyxia — 10%
acute drug toxicity — 7%
Death factors — 5 to 9 years old
drowning (all types) — 31%
trauma (motor vehicle) — 31%
other — 23%
blunt force trauma — 15%
Death factors — 10 to 14 years old
trauma (motor vehicle) — 41%
other — 27%
drowning (all types) — 18%
asphyxia — 14%
Death factors — 15 to 19 years old
trauma (motor vehicle) — 46%
acute drug toxicity — 27%
other — 17%
drowning (all types) — 10%
Among infants and toddlers aged 0 to 4 years, accidental drowning was the most common death factor. Both accidental drowning and trauma from motor vehicle–related injuries were the most common manner of death among children between the ages of 5 to 14 years. For youths aged 15 to 19 years, trauma from motor vehicle–related injuries was the highest contributing factor for accidental deaths, followed by acute drug toxicity.
Child and Youth Death Review and Analysis (CYDRA) Unit
Overview
The OCC has been collaboratively working over the recent years to enhance child and youth death investigation and review. The Child and Youth Death Review and Analysis (CYDRA) Unit within the OCC has been developing and transforming processes for child and youth death review. This transformation has been informed by engaging and collaborating with individuals and organizations, whose perspectives have been insightful, beneficial, and valuable.
CYDRA investigates and reviews the unfortunate deaths of children and youth. The unit reviews deaths in a respectful and inclusive way, acknowledging the journeys of children and youth, and their unique identities. The CYDRA review process aims to fully understand the circumstances of the deaths and analyzes how various support systems intersected with the young person.
CYDRA’s focus is generating policy recommendations with a purpose to highlight service issues as well as systemic and structural inequities. Recommendations are issued to agencies and organizations in various sectors, as well as provincial ministries and federal departments. CYDRA team members are not death prevention experts, rather the unit’s work informs death prevention efforts through knowledge mobilization and sharing of lessons learned. The OCC does not have the legislative authority to make findings of guilt or blame or imply responsibility on any person(s) or agency, organization or other entity.
The unit continuously engages with Indigenous communities and organizations, with feedback incorporated into CYDRA’s death review process. Working directly with Indigenous communities serves to challenge colonial approaches and supports CYDRA’s work to generate relevant and meaningful recommendations.
The following principles underpin the work of CYDRA:
Equity: Mindful of the legacies of colonialism, oppression, racism, and discrimination perpetrated against equity–deserving groups.
Respect: Honour the journeys of loved ones by humanizing the review process and demonstrating compassion given the grief and trauma that their family members, communities and service providers experience.
Inclusivity: Find creative ways to involve families, communities, agencies, institutions, and people who had an influence or were influenced by the life and/or death of the child or the young person.
Intersectionality: The understanding that an individual’s life experiences and outcomes are largely defined by the aggregated impact of their unique identities and their interaction with various support systems.
Integrity: Staying true to CYDRA’s purpose and processes, maintaining fairness in allocation of resources, while being flexible to customize, as needed.
Humble / Realistic: Accurately communicate the function CYDRA performs and its limitations in compelling system change and recognizing the limitations of death review processes and analyses.
CYDRA death review continuum
Recognizing that death prevention is a shared responsibility, and that children, youth, families, and communities are impacted by multiple systems, the death review process aims to understand how these systems intersect. Multiple perspectives at various levels help to inform death investigations and reviews. With broader input and participation, there will be increased opportunity for timely, relevant learning for all to inform the prevention of child and youth deaths.
Many of the deaths that CYDRA reviews are reported or referred in one of two ways:
- The 2006 Joint Directive on Child Death Reporting and Review. This directive is issued under section 20.1 of the Child and Family Services Act and replaces the October 1, 2000 joint directive on child death reporting and review outlines the process that children’s aid societies and Indigenous child and family well–being agencies must follow when reporting and reviewing child and youth deaths. The Directive applies when either:
- a child who was receiving service from a society/agency at the time of their death, dies
- a child who received service from a society/ agency at any time in the 12 months prior to the death, dies
- Deaths are also referred to the CYDRA Unit by a coroner, or at times by an individual or organization.
CYDRA’s review process is best characterized as a review continuum. Each death that is reported or referred to CYDRA is reviewed, with some moving further along the review continuum. Deaths with no child welfare involvement are also reviewed by CYDRA where service, systemic or structural issues are identified. CYDRA will continue to use existing mechanisms to gather important information from sectors and organizations other than child welfare, as part of a comprehensive death review process.
The current review process includes collaborations with family, First Nation participants (including Elders and Knowledge Keepers) and communities, with further development of community–specific protocols. There is a focus on multisectoral intersections and various service systems. To increase access, reviews can be held virtually, in–person at a central location, or in community. Finally, membership at a review table will be dynamic, with review participants determined based on community input, circumstances of death, and involved systems.
CYDRA review transformation
CYDRA has implemented changes in the approach to completion of reviews. The process continues to be collaboratively transformed and customized to best serve the purpose of a death review and increase cultural safety. Chart 7 outlines the transformation of the review process over recent years.
Chart 7: CYDRA process transformation and comparison
- Historical PDRC - CW Process
- Fixed membership / standing committee
- Reviews / meetings held centrally in Toronto
- Focused on child welfare system only
- No family notification / involvement / input
- No collaboration with communities (for example FNIM)
- CYDRA’s Process
- Dynamic input based on unique circumstances, community input, the involved systems, etc.
- Reviews held virtually or in the community (local)
- Multisectoral focus that includes intersections / various service systems
- Collaboration with / input from family
- First Nation communities are engaged early, involved in planning, participate in review
Child welfare – society/agency involvement
The majority of child and youth deaths reviewed by CYDRA are those that are reported to the OCC under the 2006 Joint Directive on Child Death Reporting and Review. Child welfare services in Ontario are provided by 13 Indigenous child and family well–being agencies, and 37 children’s aid societies.
Use of data pertaining to children/youth with society/agency involvement
This report presents descriptive statistical analyses of the data arising from the investigation of deaths from 2022 and 2023 to compare and observe the child and youth population in Ontario in the context of society/agency involvement. The data analyzed over recent years suggest that there is sufficient variability year–over–year to merit the ongoing examination of the data prior to drawing any conclusions. We strive to improve our data collection mechanisms to develop larger data sets which would allow us to identify trends or provide observations previously limited by insufficient data points.
In some cases, no statistical analysis could be completed because of limitations arising from the nature of the data, the size of the populations, or challenges with data as discussed above. There are several challenges with the data available for analysis that merit consideration when reading this report.
The lack of comparator data from other sources is another significant barrier to inferential and comparative analyses. Data from different sources are collected with varying sets of parameters, depending on the organization’s needs. Some of the data required for effective comparison are unavailable. For example, having complete data related to those who are living (on factors such as health, education, social economic status, etc.) as a comparison would support the understanding of underlying factors that impact the overall well–being of children and youth, and what might contribute to the prevention of death.
CYDRA data analysis
This section of the report contains analyses on the deaths of children and youth where a children’s aid society or an Indigenous child and family well–being agency had been involved with the child, youth, or family at the time of their death or within 12 months prior to the death. This includes youth that are older than 19 years of age. Chart 8 contains the age breakdown for the deaths included in the following part of the report.
| Year | Age: 0–19 years | Age: 20 plus | Total (all ages) |
|---|---|---|---|
| 2019 | 104 | 5 | 109 |
| 2020 | 80 | 2 | 82 |
| 2021 | 101 | 16 | 117 |
| 2022 | 106 | 8 | 114 |
| 2023 | 106 | 14 | 120 |
Understanding the role of natural deaths with child welfare involvement and deaths still under investigation
CYDRA receives notification for some deaths that are from natural causes, have occurred in a hospital/hospice, or that were expected to occur, which under normal circumstances would not likely be investigated by a coroner. These deaths are excluded from the analyses undertaken in this report to allow for the comparison of deaths with society/agency involvement against the cohort of children and youth coroner investigations (which does not include natural deaths free of care–related concerns). In 2022 and 2023, 29 child and youth deaths fell into this category and have been removed from the following analyses.
In 2022 and 2023 combined, CYDRA received a total of 272 death notifications from societies/agencies, and 9 additional referrals from Regional Supervising Coroners (all deaths either without child welfare involvement or which didn’t meet the criteria for reporting under the joint directive). After reviewing all of them, 38 deaths were excluded for the purposes of this report. The specific exclusion criteria can be found in the data notes in Appendix A.
Chart 9: Children and youth deaths with and without society/agency involvement in 2023
- Total Ontario deaths (ages 0-19): 1,139
- Coroners investigation (ages 0-19): 1,139
- society involvement (age 0-24): 132
- in care: 8
- not in care: 112
- Ready, Set, Go/CCSY/VYSA: 12
- customary care: 12
- natural hospital deaths: 12
- no society involvement: 400
- regional supervising coroner referrals: 5
Chart 9 presents a breakdown of the death notifications CYDRA received in 2023. In total there were 132 deaths of children and youth that were reported to CYDRA, and 5 additional referrals from Regional Supervising Coroners. Twelve of these deaths were excluded from our analysis as they were determined to be natural hospital deaths. There were 8 deaths that occurred while the child or youth were in care of the society/agency, and 112 that were not in care.
Chart 10: Number of deaths of children and youth by age group with society/agency involvement, 2019–2023

In 2023, the highest number of deaths with society/agency involvement were among infants and toddlers between the age 0 to 4 years, followed by youth between 15 and 19 years for both 2022 and 2023. This pattern has been consistent since 2019.
In 2023 there were 14 deaths, compared with 8 deaths in 2022 among the age group 20 plus years. This is likely attributable to new child welfare program criteria resulting in increased notifications for this age group.
Chart 11: Number of deaths of children and youth by manner of death with society/agency involvement, 2019–2023*

*Please note that one death from 2022 and nine deaths from 2023 were not included in Chart 11 as they were under investigation at the time of this report.
In 2019 and 2020, undetermined was the most common manner of death among children and youth, however from 2021 to 2023, accident was the most common manner of death. Homicide was consistently the least common manner of death in the five–year period, followed by suicide.
Deaths due to acute drug toxicity
Similar to observations observed with all children and youth investigated by the OCC, accident was the most common manner of death among children and youth with society/agency involvement for both years. In 2022, 16% and in 2023, 21% of all deaths resulted from acute drug toxicity. Although majority of these deaths were determined to be accidental, the manner of death in some instances were suicide or undetermined.
Children and youth in care aged 0–17
Children and youth were included as being in care when they were identified by the society/agency as having one of the following legal statuses:
- interim society care
- extended society care
- subject of a temporary care agreement
- in temporary care and custody/interim care and custody
Children and youth who are legally in care may have different living arrangements, including residential care (family–based or group), temporarily staying with family, or living independently at the time of death.
Customary care
A child or youth in Customary Care is a First Nations, Inuit, or Métis young person, legally in the care of a person who is not the child’s parent, according to the custom of the child’s band, First Nation, Inuit or Métis community.
Child welfare services for youth aged 16–17
Voluntary Youth Services Agreement (VYSA) is an agreement between a society and a youth who is 16 or 17 years old, for services and supports to be provided for the youth. Service is provided where youth meet the criteria and wants to work with the society/agency voluntarily.
Youth in the Ready, Set, Go (RSG)/Continued Care and Support for Youth (CCSY) programs
In April 2023, the Ready, Set, Go (RSG) program was introduced to replace the Continued Care and Support for Youth (CCSY) program. The intent of the RSG program is to provide supports to youth transitioning out of care with life skills and support their need to pursue post–secondary education, skilled trades training, and employment opportunities. Ontario Connecting Youth Leaving Care with Supports to Succeed, Support for youth in the child welfare system
In 2022 and 2023 there were 37 youth in the CCSY or RSG programs at the time of their death or who were receiving services in the 12 months prior to their death. The youth were of age 18 years and above.
| Manner of death | 2022 | 2023 |
|---|---|---|
| Accident | 9 | 12 |
| Homicide | 3 | 1 |
| Natural | 2 | 2 |
| Suicide | 2 | 3 |
| Undetermined | 1 | 2 |
| Total | 17 | 20 |
In the two years combined, accident was the most common manner of death among deaths in this age group. Out of the 21 accidental deaths, 19 of the deaths resulted from acute drug toxicity.
Deaths of First Nations children and youth with society/agency involvement investigated by the Office of the Chief Coroner
CYDRA is collaboratively developing ethical data governance approaches for Indigenous identity–based information recorded in death investigations which honour community perspectives. Although deaths among First Nations, Métis, and Inuit children and youth are included in this report’s aggregate data, the report does not present data that is specific to Métis and Inuit children and youth. Information relating to the deaths of First Nations children and youth investigated by the OCC are presented below.
The ability to undertake meaningful analysis of the deaths of First Nations children and youth served by societies/agencies is affected by limited data available to the OCC. During the death investigation process, First Nations ancestry of children and youth may not be determined. Coroners may not identify children and youth as First Nations as they rely on the information available during their investigation (information sources include but are not limited to family members, community service providers, and police services). This affects the determination of an accurate number of First Nations children and youth deaths that were investigated by the OCC.
For the purposes of this analysis, children and youth were identified as First Nations when any Indigenous child well–being agency or any non–Indigenous children’s aid society made note of their First Nations heritage in information provided to CYDRA. Children and youth were also identified as First Nations by the investigating coroner.
Summary information using available data has been provided; however, given the noted limitations, meaningful inferences cannot be made. It is important to note that although these data are being shared, findings and conclusions should not be drawn from the data. The OCC is presenting these observations while acknowledging the limited data available. Specific understanding of First Nation child and youth deaths is attained by collaboratively working with First Nations communities. CYDRA will continue to co–develop, with First Nation communities, the approach to systemic reviews. This has and will continue to support culturally–safe processes, accurate and comprehensive understanding, as well as recommendations that are informed by, and relevant to, community contexts.
The OCC and CYDRA anticipate that as death investigation and review processes improve, the quality and availability of data regarding Indigenous children and youth will be enhanced. Working directly with communities, analyses will more effectively inform prevention strategies targeted to Indigenous children and youth.
Analysis –First Nations children and youth
Between 2022 and 2023, there were 56 deaths of First Nations children and youth between the ages of 0 and 23 years that had a society/agency involvement at the time of their death or 12 months prior.
Chart 13: Number of deaths of First Nations children and youth with society/agency involvement by age groups, 2022–2023

Chart 13 displays the number of deaths of First Nations children and youth with society/agency involvement broken down by age groups. In 2022, the highest number of deaths were among youths between the ages of 15 and 19 years, followed by infants and toddlers of ages 0 to 4 years. Although the overall number of deaths in 2023 was lower, the distribution across the age groups followed a similar pattern as 2022, where the highest number of deaths were among infants and toddlers and youths between the ages of 15 and 19 years.
Chart 14: Deaths of First Nations children and youth with society/agency involvement by manner of death, 2022–2023*

*Please note that one death from 2022 was not included in this chart as it was under investigation at the time of this report.
In 2022, accident was the most common manner of death, which accounted for 59% of the deaths among First Nations children and youth with society/agency involvement. Similarly, in 2023, accidents accounted for 45% of all deaths among this population. In the two years combined, the most common death factors were acute drug toxicity, drowning, and asphyxia due to hanging, which accounted for 43% of all the deaths.
Recommendations
In 2022 and 2023, CYDRA issued over 50 recommendations formulated from completed death reviews and identification of trends in data. These recommendations were issued to various sectors and organizations as shown in chart 15.
Chart 15: Sectors and organizations recommendation recipients in 2022–2023
- Child Welfare
- Children's aid societies / Indigenous child & family well-being agencies
- Ontario Association of Children's Aid Societies
- Association of Native Child and Family Services Agencies of Ontario
- Provincial Ministries
- Education
- Children, Community and Social Services
- Health
- Attorney General
- Municipal Affairs and Housing
- Professional Colleges
- Psychologists
- Social Workers and Social Service Workers
- Psychotherapists
- Teachers
Recommendations were issued to organizations within three main categories –child welfare, provincial ministries, and professional colleges. These recommendations were then analysed to identify themes and patterns. Chart 16 further categorizes the recommendations into themes within five categories.
Chart 16: Thematic analysis of all the recommendations issued in 2022 and 2023.
Service level community collaboration
Service coordination → community intervention/development
Staff education/training
Family violence → human trafficking → 2SLGBTQ+ → supervisor training
Organizational focused
Practice and protocols → guidelines/standards → service delivery
System-level change
Inter-ministerial collaboration → policy development/changes → funding enhancement
Family/youth support
Access to mental health services → enhanced youth support → cultural safety
Community Engagements
CYDRA engaged with Indigenous and non–Indigenous communities to better understand how current death investigation and review processes could be enhanced, and how deaths may be prevented. Feedback continues to be incorporated into the OCC’s and CYDRA’s processes. We have provided examples of engagements that took place in 2022 and 2023.
Awareness Days July 2022
In July 2022, CYDRA hosted a two–day awareness event to discuss the interim death review processes and policy initiatives led by the unit. This event brought together agencies, organizations, and other ministries across the province to learn about trauma–informed practices, anti–Indigenous racism, anti–Black racism, and anti–oppression theory and practices, as well as various initiatives and practices.
Anishinabek Nation
The OCC worked with Anishinabek Nation (AN) to conduct community engagements related to child and youth death review processes. The work began in 2023 continuing into 2024 with several virtual and in person sessions with community–based service providers from AN–member communities. The OCC and CYDRA listened to all the feedback and learned about cultural safety in death investigation and review processes. A formal report was submitted to the OCC containing insights and recommendations brought forward during each engagement to improve the death investigation and review process for loved ones from AN communities. The OCC is at the beginning stages of reviewing and planning for implementation of the recommendations in collaboration with AN.
Nishnawbe–Aski Nation
In May 2023, the CYDRA team supported community engagement with a number of Nishnawbe–Aski Nation (NAN) communities. This was CYDRA’s first formal engagement with NAN communities with the intention of building relationships and initiating protocol development for the death review process. The discussion at the gathering focused on a number of areas:
- Putting child and youth lives first, bringing their voices forward along with the voices of their families and communities.
- Death review processes need to include communities, take a systems approach, focus on understanding the circumstances of deaths and what needs to change. Community–specific protocols were envisioned as a way forward.
- The importance of culture, traditions and ceremony, which vary from community to community, as part of the death review process. Spirit journeys can be impacted when the family/community is not notified of the death immediately, or when death investigation processes may cause additional trauma.
- The impacts of colonialism, racism, and intergenerational trauma continue, while healing and re–connection to the land can help prevent deaths.
- How past recommendations may not have resulted in needed change.
- The OCC’s commitment to continue listening and learning from First Nations leadership, Elders, communities, families, youth and children.
Follow up work continues into 2024 as CYDRA works collaboratively with NAN, service providers, and a local consultant to determine next steps.
Association of Native Child and Family Services Agencies of Ontario (ANCFSAO) Indigenous Child and Family Well–Being Conference Workshop
In 2022, the Association of Native Child and Family Services Agencies of Ontario (ANCFSAO) hosted their annual Indigenous Child and Family Well–Being Conference. CYDRA facilitated a workshop to engage in dialogue about the interim death review process and discussed the path forward and what is needed to continue the path of collaborative transformation. The open discussions were to amplify voices and celebrate the positive work being done to build and strengthen the well–being of Indigenous children and families. CYDRA is committed to informing the prevention of child and youth deaths by focusing on systems and structural inequities, along with enhancing death review processes in meaningful and inclusive ways.
Regional focus
After reviewing and analyzing deaths from one of the OCC regions, it was noted that four infants had passed away within a span of three years due to accidental drug toxicity. The tragic deaths of these infants highlighted issues related to parental substance use, housing instability, exposure to adult conflict, and intersections with the criminal justice system. The children’s aid society (CAS) in the region was engaged and held a community forum with other agencies including public health, hospital staff, police services, and other care providers. The forum identified potential improvements in current practices, services, and programs to protect young children who are at high risk of exposure to substances in the home. The outcome was the society taking the lead to build a tool which would assist with assessing risk in these situations.
Ontario College of Social Workers and Social Service Workers presentation
In June 2023, the Chief Coroner for Ontario and the CYDRA Unit Manager spoke at an annual education session for the college. The educational session aimed to inform social workers and social service workers about CYDRA’s interim process for reviewing child and youth deaths and to highlight ongoing policy initiatives led by the unit. After the presentation, there was a question–and–answer period that focused on the trends and intersections between science and social policy.
Conclusion and the way forward
The approach to child and youth death reviews has seen significant transformation over recent years. The OCC has heard and recognized concerns about the historical processes of pediatric death review that focused on child welfare services. CYDRA continues to move forward with implementing a wholistic model that incorporates the impacts of intersecting systems and inequities across service sectors.
A wholistic model provides an opportunity to better understand the unique journeys and deaths of children and youth. It supports the exploration of themes, similarities, and differences through the analysis of both quantitative and qualitative data. The purpose is to gain a comprehensive understanding of the intersecting factors, issues, systems, and structures that may have contributed to the circumstances of children and youth who have died. This understanding will help generate recommendations that are meaningful, actionable, and directed to the appropriate ministries and organizations, and to help inform the prevention of deaths.
CYDRA continues to learn about the best way forward, and values the opportunity to listen and collaborate, while reflecting on different perspectives and feedback. The OCC will continue to take action, enhancing child and youth death reviews, conducting robust analyses, and sharing the lessons learned. The OCC looks forward to continued collaborative work with many individuals, groups, organizations and governments. Together, we can help to improve public safety and inform the prevention of child and youth deaths in Ontario.
Appendix: Data sources and data notes
Data Sources
- Coroner death investigation case management systems, Ontario Office of the Chief Coroner. Extracted August 15, 2024
- Statistics Canada. Table 13–10–0709–01, Deaths, by age group and sex, last accessed December 2024
- Historical Population Estimates, Analysis for 2023, Ministry of Finance. Extracted September 2024
Exclusion criteria
This section outlines the exclusion criteria to create the cohort for the analysis of this report. Any deaths that met any of the following criteria were excluded from the cohort:
- Missing age
- Date of birth or death was missing
- Where death factor was listed as skeletal remains, stillbirth or pre–term pregnancy loss
- Natural hospital deaths
Contacts
Child and Youth Death Review and Analysis Unit
CYDRA@ontario.ca
Media inquiries:
Stephanie Rea
Issues Manager
Office of Chief Coroner, Ministry of the Solicitor General
Stephanie.Rea@ontario.ca
Any person seeking to reproduce data or information from this report is asked to contact the Office of the Chief Coroner to ensure accuracy.