2018 deaths with society involvement — status of children and youth
Consistent with findings in previous years, 84% (106/126) of the children and youth that died in 2018, where a Society was involved with the child, youth or family within 12 months of the death, were not in the care of a Society at the time of their death. This includes seven youth (aged 19-21) that were receiving Continued Care and Support for Youth (CCSY) from a Society, which a youth in care may be eligible to receive when their care and/or custody order expires upon their 18th birthday, as well as those who died of natural causes whose deaths would not have been investigated if they were not receiving services from a Society. Excluding those who died from natural causes that would not have otherwise been investigated as well as those over the age of 18, 85% (82/97) were not in care at the time of their death. Of the 15% (15/97) of these children and youth that were in the care of a Society, three were in customary care, four were in extended Society care, five were in temporary Society care, one was subject to a temporary care agreement, one had a voluntary youth services agreement and one was in residential care for medical reasons.
What does the available data tell us?
Information provided by the Societies through Child Fatality Case Summary Reports supports a greater understanding of the circumstances surrounding the deaths of children and youth. In particular, the information helps to illuminate particular risks and vulnerabilities. The information below summarizes information received from the society(ies) involved with the child/youth. There is one cases for which information is pending.
- In 2018, 95 (75%) of cases where a child or youth, including those receiving CCSY that had been receiving services from a Society were open files at the time of death (see Chart 17). This is consistent with previous years.
- 37% of the cases in 2018 were rated as high or very high risk at the time of death (see Chart 18). The Ontario Child Protection Standards released in February 2016 require that when deciding whether more frequent visits are required the worker considers:
- the risk rating on the risk assessment;
- the strengths and needs of the family;
- whether a safety plan is actively being monitored and the child continues to reside in the home; and
- the vulnerability of the child.” (Standard 7, page 83).
- Requirements of the Standards would suggest that in these cases, the Society would have been engaging with the family with some frequency prior to the death.
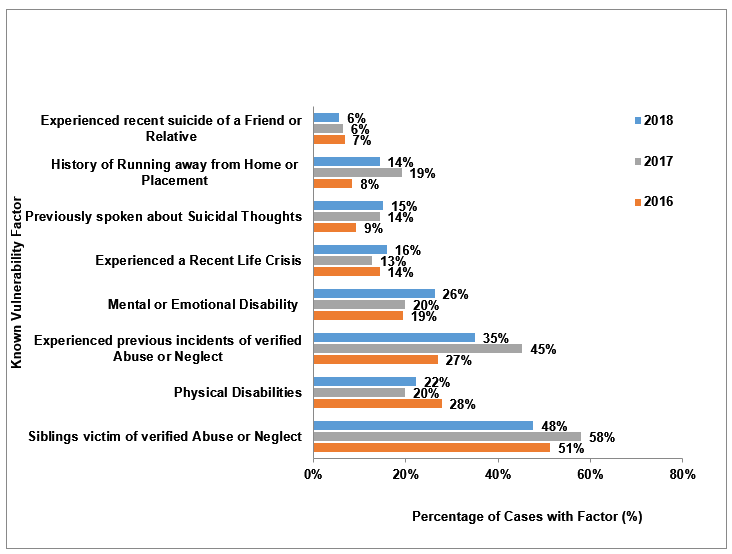
- A history of verified abuse and neglect of the child or youth and/or the sibling(s) of the deceased continued to be the most commonly reported vulnerability factor (see Chart 19). 35% of society reports in 2018 regarding the deaths of children and youth indicated that the child or youth had been the subject of verified abuse or neglect, and in 48% of cases reported in 2018 indicated that a sibling of the child or youth had been the subject of verified abuse or neglect. In 28 cases (22%) reported in 2018, both of these vulnerability factors were present.
- Disabilities are the next most commonly reported vulnerability factor (see Chart 19). 22% of the children and youth that died in 2018 had physical disabilities, and 26% in 2018 had mental or emotional disabilities. In 4% of cases in 2018, both of these vulnerability factors were present. Chart 19 provides a comparison of 2016 through 2018 data on vulnerability factors reported by societies.
- Suicide was the manner of death for 17 youth receiving services from a society (ages 0-18) and three of the youth who received CCSY in 2018 (aged 19-21). Of these, three were Indigenous youth. There are three known or suspected vulnerability factors related to suicide reported on the Child Fatality Case Summary Report by societies – child/youth has previously attempted suicide, recently experienced the suicide of a friend or relative, and/or had spoken to someone about suicidal thoughts. For eight of the 20 youth, there was more than one of these vulnerability factors present. In 2018, eight youth had previously attempted suicide, 12 had previously spoken to someone about suicidal thoughts and three had recently experienced the suicide of a friend or relative.
Chart 17 shows the case status for Society involved cases of children and youth between the ages 0 – 21 that died in 2018, which includes individuals who were receiving Continued Care and Support for Youth at the time of their death. 75% of cases were open at the time of the death, and 25% of cases were closed at the time of the death but had been open in the 12 months preceding the death.
Chart 17: Case status at the time of death – Society involved cases in 2018 (n=126)
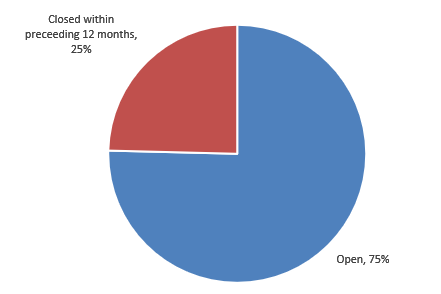
Chart 18 illustrates the risk rating reported by the Society at the time of death or case closure for Society involved cases in 2018. 11% of the cases were rated very high risk, 26% of cases were rated as high risk, 27% moderate risk, 6% low risk and 30% were categorized by the reporting Society as “not applicable”.
Chart 18: Overall risk rating at time of death/case closure – Society involved cases in 2018 (n=126)
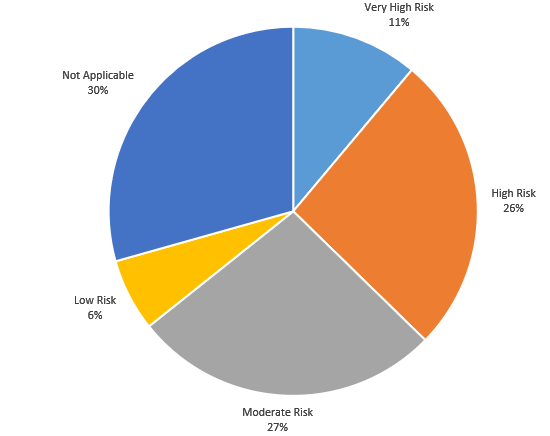
Chart 19 illustrates the proportion of 2016, 2017 and 2018 cases with Society involvement of children and youth aged 0-21 where the Society reported known vulnerability factors. As in previous years, in 2018, verified abuse and neglect of the child or youth that died and/or their sibling were the most commonly reported vulnerability factors. Mental or emotional disabilities were the next most commonly reported vulnerability factor, followed by physical disabilities.
Chart 19: Known vulnerability factors – Society involved cases 2016-2018
While the information that the Society provides when a child or youth dies is valuable in identifying particular vulnerability factors, there may be other risk factors for children and youth that are not reported through the Joint Directive reporting process. This is because all potential risk factors for children and youth in Ontario are not collected in a standardized way. Furthermore, the factors collected should not be construed as unique to children and youth that have died, or to children and youth that were receiving the services of a Society. It is not known whether the prevalence of identified factors is different in the population of children and youth that have died as compared to the living population of children and youth in Ontario or receiving services from a Society.