Part 2: Occupational cancer in Ontario
Setting the context
The Canadian Cancer Society has estimated that 82,100 Ontarians will receive a cancer diagnosis in 2019 and that 29,700 will die from cancer (4). Looking to the future, unless we make progress in prevention and treatment, approximately 44% of us will be diagnosed with cancer in our lifetime and 24% of us will die of cancer. Based on what is currently known about the causes of cancer, it has been estimated that approximately half of all cancers, including those caused by work, are preventable (5, 6).
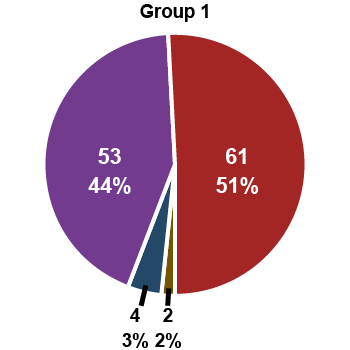
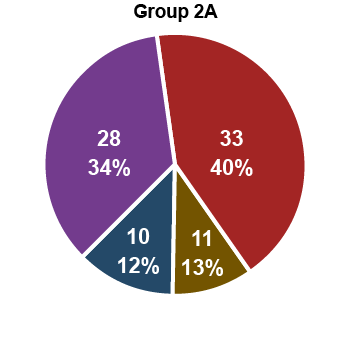
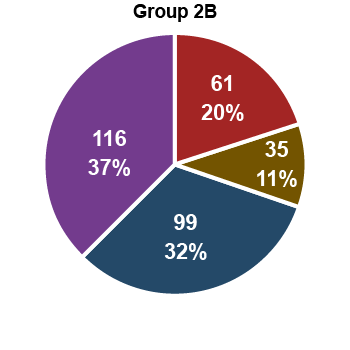
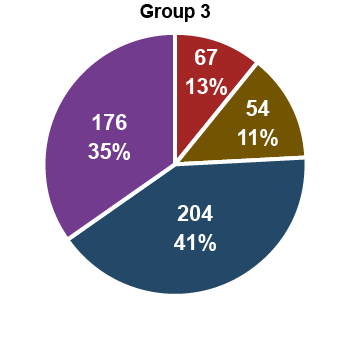
While there is still much that we do not know about the causes of cancer, many workplace carcinogens have been identified. A recent paper by researchers from the International Agency for Research on Cancer (IARC), which has a program to classify the carcinogenicity of suspected agents, identified 47 Group 1 (definite) carcinogens that were classified on the basis of workplace evidence of carcinogenicity (7). Expanding on this analysis, the Occupational Cancer Research Centre (OCRC) has identified 63 IARC Group 1 and 44 IARC Group 2A (probable) workplace carcinogens based on epidemiologic or exposure studies cited in the monographs as of July 2019 (Figure 1) (8).

The impact of occupational carcinogens in Ontario
Hundreds of thousands of Ontarians have been exposed to a wide range of known and suspected carcinogens in the workplace. However, the impact of these exposures on health is not always clear. In order to answer this question, the OCRC started the Burden of Occupational Cancer Project
As shown in Table 1, approximately 3,000 cancers diagnosed each year in Ontario are due to occupational exposure to 16 carcinogens commonly found in the workplace (10).
| Carcinogen | Annual cancers in Ontario (Note 1) | Currently exposed (Note 2) |
|---|---|---|
| Solar UV at work | 1400 non-melanoma skin | 449,000 |
| Asbestos | 630 lung, 140 mesothelioma, 15 larynx, <5 ovarian, additional colorectal and stomach | 52,000 |
| Diesel exhaust | 170 lung, 45 bladder | 301,000 |
| Crystalline silica | 200 lung | 142,000 |
| Welding fumes | 100 lung | 169,000 |
| Nickel | 80 lung | 48,000 |
| Chromium VI | 25 lung | 39,000 |
| Secondhand smoke at work | 50 lung, 10 pharynx, 5 larynx (Note 3) | 125,000 |
| Radon | 60 lung | 34,000 |
| Arsenic | 20 lung | 8,000 |
| Benzene | 10 leukemia, <5 multiple myeloma | 147,000 |
| PAHs | 60 lung, 15 skin, 30 bladder | 134,000 |
| Shiftwork | 180-460 breast | 833,000 |
| Artificial UV Radiation | 5 ocular cancer | 48,000 |
| Wood dust | <5 sinonasal, <5 nasopharyngeal | 92,000 |
| Formaldehyde | <5 leukemia, <5 sinonasal, <5 nasopharyngeal | 63,000 |
Notes to Table 1
- based on 2011 cancer statistics; IARC probable associations are in bold
- source: CAREX Canada
- among never smokers
Solar radiation, asbestos, diesel engine exhaust and crystalline silica are the occupational carcinogens with the largest impact on cancer burden in Ontario (10).
- approximately 449,000 workers in Ontario spend a significant amount of time working outdoors and are exposed to solar radiation, which causes an estimated 1,400 non-melanoma skin cancer cases annually
- although fewer than 55,000 workers in Ontario are currently exposed to asbestos at work, past exposure is responsible for 630 lung cancers, 140 mesotheliomas, 15 laryngeal cancers and fewer than 5 ovarian cancers annually in the province. Asbestos exposure may also be responsible for additional colorectal and stomach cancers, but the project was not able to estimate the number
- diesel engine exhaust exposure, which currently affects about 301,000 Ontario workers, accounts for 170 lung and a suspected 45 bladder cancer cases each year
- crystalline silica causes approximately 200 lung cancer cases each year and there are an estimated 142,000 Ontario workers currently exposed
The economic analyses for the study, which were led by the Institute for Work & Health, looked at direct costs (i.e., healthcare costs, out-of-pocket costs, insurance administration, and informal caregiver costs), indirect costs (i.e., productivity/output costs and replacement costs for ill workers), and intangible costs (i.e., monetary value of the loss of health-related quality of life). The economic estimates represent the total lifetime costs of newly diagnosed cancers in Canada (based on the reference year of 2011).
- the estimated costs per case of mesothelioma and lung cancer were approximately $1.1M and $1.0M, respectively (9)
- the estimated cost for each case of occupational bladder cancer was $660,000 (11)
- the estimated cost for each case of non-melanoma skin cancer differed between squamous cell and basal cell carcinomas ($10,600 vs. $5,700, respectively) (12)
- economic burden estimates can also be made for specific exposures. For example, the economic burden for lung cancer and mesothelioma due to asbestos exposure in Canada added up to $831 million in direct and indirect costs for newly identified cases and $C 1.5 billion in quality of life costs (13)
It is important to point out that these are not the costs to the compensation system, but costs measured at the societal level.
The number of cancers that are currently compensated in Ontario
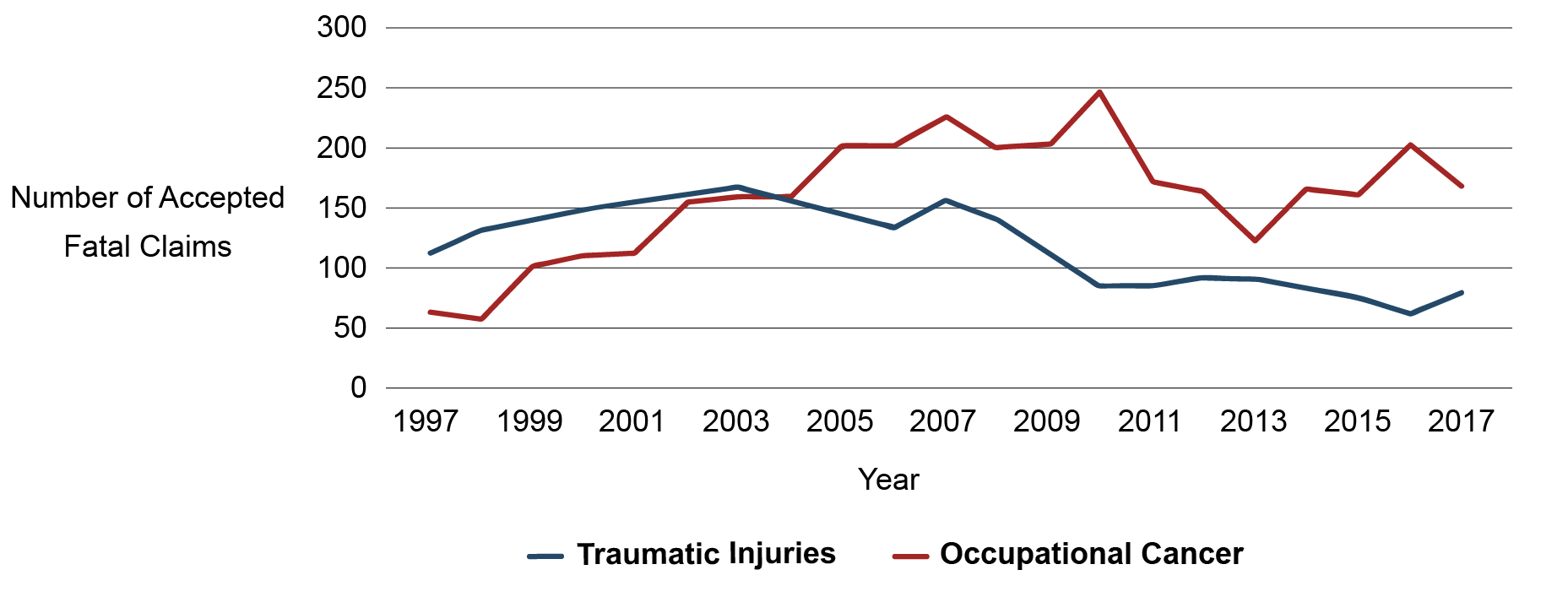
In 2013, the OCRC published a report that used data from the Association of Workers' Compensation Boards of Canada (AWCBC) to describe trends in compensated claims for deaths from occupational cancer in Ontario and Canada overall for the period 1997–2010 (14). Compensated claims for deaths from occupational cancer have increased dramatically over that period, surpassing those for traumatic injuries in Canada. The change was particularly dramatic in Ontario where the number surpassed injuries in 2005 and, by 2010, there were more than twice as many fatal cancers compensated. The analysis was extended to 2017 for this report (Figure 2). Although the number fluctuates from year to year, the data demonstrate that there are still many more fatal cancer claims accepted annually than traumatic injury claims.
Figure 2: WSIB accepted workplace fatalities (1997–2017)
Fatal claims, however, only represent part of the cancer picture. Data provided by the WSIB on all cancer claims
| Primary cancer | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mesothelioma | 90 | 79 | 88 | 70 | 73 | 80 | 66 | 78 | 76 | 62 | 762 |
| Lung cancer | 87 | 75 | 56 | 62 | 45 | 48 | 71 | 45 | 54 | 53 | 596 |
| Other cancers | 49 | 38 | 41 | 32 | 27 | 17 | 17 | 20 | 32 | 47 | 320 |
| Total | 226 | 192 | 185 | 164 | 145 | 145 | 154 | 143 | 162 | 162 | 1,678 |
| Agent | Cases |
|---|---|
| Asbestos | 1291 |
| Crystalline silica | 23 |
| Benzene | 21 |
| Defoliants and herbicides | 38 |
| Solar & ultraviolet radiation | 24 |
| Coal Tar | 14 |
| Foundry emissions | 13 |
| Coke oven emissions | 11 |
| Nickel & sinter plant emissions | 18 |
| Welding fumes | 9 |
| Uranium (radon) | 8 |
| Exhaust gases - diesel | 7 |
| Rubber chemicals | 6 |
| Ultraviolet radiation | 6 |
| Solvents | 6 |
| Aluminum powder | 6 |
| Trichloroethylene | 5 |
| Ionizing radiation | 5 |
| Aromatic hydrocarbons | 5 |
| Other and unspecified agents | 172 |
The gap between the estimated burden and what is compensated in Ontario
Comparing the data in Table 1 and Table 3 (above) reveals that claim statistics do not reflect the estimated true number of occupational cancers in Ontario. Cancers due to asbestos exposure were the most well compensated category between 2009 and 2018, with an average of approximately 130 cases compensated each year (Table 3). Of these, approximately 80 were for mesothelioma (Table 2). However, based on the reference year of 2011, the Burden of Occupational Cancer Project estimated that occupational asbestos exposure caused 630 lung cancers and 140 mesotheliomas (and smaller numbers of larynx, ovary, colorectal and stomach cancers) in Ontario (Table 1) (13). Similar discrepancies are observed in the number of predicted cases vs. the number of accepted claims for exposure to solar UV radiation (1,400 predicted vs. 24 accepted), diesel engine exhaust (170 predicted vs. 7 accepted), crystalline silica (200 predicted vs. 23 accepted) and welding fumes (100 predicted vs. 9 accepted). Based on well-established associations, a total of 2,900 cancer cases are predicted overall for the 16 carcinogens listed in Table 1 compared to the average of 170 accepted claims per year. It is important to point out that only a fraction of this gap is explained by rejection of claims, given that only 400 claims are filed per year and many of these are for associations not on the IARC list.
How Ontario compares to other jurisdictions
Ontario vs. other Canadian provinces
To compare compensation in Ontario to other provinces, we calculated the claims rate per 100,000 workers, using data from the AWCBC on accepted fatal claims and a report on the scope of labour force coverage (15). Based on AWCBC data, there were 161 fatal cancer claims in Ontario in 2015, resulting in a claim rate of 3.1 per 100,000 covered workers. The overall claim rate for Canada that year was 2.5, which was similar to BC (at 2.4), Quebec and Manitoba (both at 2.5). Newfoundland and Labrador had the highest rate (at 5.2), while Alberta had the lowest (at 1.2) and the remaining provinces (which had too few cases to report individually) had a combined rate of 2.0 claims per 100,000 insured workers. Based on AWCBC data, mesothelioma due to asbestos exposure was the dominant fatal cancer compensated in Canada, comprising 46% of all claims. Mesothelioma accounted for 36% of the fatal claims in Ontario and Alberta, for 58% in Quebec, and for 65% in BC.
The Burden of Occupational Cancer Project estimates that there almost five asbestos-related lung cancers for every mesothelioma and our findings indicate that these are both severely under-reported and under-compensated. There are a number of factors that potentially impact compensation, such as provincial policies and the recognition of causality by clinicians. In 2016, the OCRC conducted a small analysis to investigate the impact of these factors on compensation for fatal mesotheliomas and lung cancers due to asbestos (16). To calculate the proportion compensated, we divided the mean number of compensated fatal asbestos cases for the period 2011–2014 (determined from AWCBC data) by the number of estimated fatal asbestos cancers in 2011 from the Burden of Occupational Cancer Project. The overall results showed that 61% of mesotheliomas and 5% of lung cancers due to asbestos in Canada were compensated. Ontario's results were 61% and 6%, respectively. Among the other provinces, only BC was substantially better for mesothelioma, with virtually all cases being compensated at that time. For lung cancer, Quebec and BC were similar to Ontario, with the remaining provinces compensating fewer.
Ontario vs. select international jurisdictions
To compare compensation in Canada to some of the major European jurisdictions, we used data from a report entitled Incidence and detection of occupational cancer in nine European countries
, which included statistics for Germany, Austria, Belgium, Denmark, Finland, France, Italy, Sweden and Switzerland (17). In 2016, the countries with the highest rates of accepted occupational cancers claims per 100,000 insured workers were: Germany, France, Denmark, Italy, and Belgium (Figure 3). In 2018, Ontario accepted 162 cancer claims of all kinds. With a covered population that year of 5,592,000 people, the rate of accepted cancer claims in Ontario was significantly lower than all of these jurisdictions at 2.9 per 100,000 insured workers.
Figure 3: How the accepted claims rate in Ontario compares to selected European jurisdictions
Accepted claims rate, per 100,000 insured workers:
Germany
France
Denmark
Italy
Belgium
Ontario
The countries that accepted the highest percentage of submitted claims were Austria (87.2%) and France (79.1%), while Denmark accepted the lowest at 28.2%. For comparison, Ontario accepted 42% of submitted claims in 2018.
In all jurisdictions except Germany, accepted cancer claims for 2016 were driven by asbestos-related cancers. In Germany, asbestos-related cancers made up 30% of accepted claims, while in the remaining eight countries, 75% or more were asbestos-related. In Ontario, asbestos-related cancers accounted for 77% of all accepted claims in 2018. Overall, Germany, France and Italy compensated the greatest variety of cancer types. In 2015, Germany began including skin cancer caused by UV radiation on its list of occupational diseases and by 2016, the majority of accepted claims were for skin cancer (3,782 claims, or 58%). France had the second-lowest percentage of asbestos-related claims (at 75%) and it was the only country to compensate more asbestos-related lung cancer than mesothelioma.
For both Germany and France, almost all recognized cases were on the presumptive lists (see Selected international jurisdictions in Part 5 of this report). Germany recognized only 28 off-list
cancers (0.43%) while France recognized 94 (4.44%). While occupational carcinogen exposure can vary between countries based on the major industries and exposure prevention, it is interesting to note that Sweden, which does not include any cancers on its presumptive list, had a ratio of only 0.5 accepted claims per 100,000 insured in 2016, and recognized only 27 claims (out of 56 submitted, 48%).
How occupational cancer claims are compensated in Ontario
This section briefly summarizes our understanding of how claims for occupational cancer are adjudicated in Ontario and how scientific principles are currently used to inform the policy development process. While a detailed analysis of the policy and legal context for compensating occupational cancers is outside the scope of this review, we have provided a list of the WSIB’s occupational cancer policies considered in this review in Appendix 2.
In determining entitlement to compensation for occupational cancers specifically, and for occupational diseases more generally, the key adjudicative question to be resolved is that of causation. Thus, in adjudicating a claim, decision-makers seek to determine whether the disease is due to the nature of the worker's employment (i.e., is the disease work-related?). Three general principles govern how causation is evaluated and entitlement is determined:
- Employment does not have to be the predominant or primary cause. The exposure has to contribute in a significant or material way to the development of the disease, but there is no requirement in law or policy that the employment or the exposure be the only cause. To determine if the exposure was of causative significance, decision-makers are expected to apply the de minimus test (i.e., did the worker have a more than trifling amount of exposure?).
- Absolute certainty is not required. Because the standard of proof is the balance of probabilities, absolute certainty is not required to evaluate causation and to determine entitlement. Decision-makers must weigh the evidence and be satisfied that it is more likely than not that the work exposure was a significant contributing factor in the development of the worker's cancer.
- The worker is afforded the benefit of the doubt. Where the evidence for and against causation is evenly weighted, the Workplace Safety and Insurance Act, 1997 requires that the benefit of the doubt be given to the claimant and the issue be resolved in their favour
footnote 3 .
These principles apply to the adjudication of all claims, regardless of whether they are for occupational diseases, physical injuries or psychological injuries. The threshold for causation and the evidentiary burden are the same for injuries and diseases, other than those to which a presumption applies where the evidentiary burden of rebutting work-relatedness falls on the employer.
Adjudication and management of occupational cancer claims in Ontario are handled by the WSIB's Occupational Disease and Survivor Benefits Program, a unit comprised of senior adjudicators, physicians, occupational hygienists, and nurse case managers. Entitlement is determined using the following methods
Compensation of cancers presumed to be work-related
Many workers' compensation systems in Canada and around the world have presumptive lists of occupational diseases, which appear either in schedules to the legislation or in supporting regulations. If a worker is diagnosed with a disease identified in the regulated list and has worked in the corresponding activities, the disease will be presumed to be an occupational disease. While presumptions of work-relatedness are generally rebuttable (i.e., evidence to the contrary may be provided that allows the compensation board to conclude that, in the specific case of an individual worker, the disease was not attributable to work), some jurisdictions, including Ontario, have occupational disease presumptions that are non-rebuttable (i.e., evidence to the contrary is not permitted).
Under Schedules 3 and 4 of O. Reg 175/98, three cancers are afforded a presumption of work-relatedness: epitheliomatous (skin) cancer, primary cancer of the nasal cavities or of the paranasal sinuses, and mesothelioma of the pleura or peritoneum (Table 4)
| Description of Disease | Description of Process |
|---|---|
| Cancer — epitheliomatous (skin) cancer | Any process involving use or handling of tar pitch, bitumen, mineral oil or paraffin or any compound, product or residue of these substances
|
| Cancer — primary cancer of the nasal cavities or of paranasal sinuses | Concentrating, smelting or refining in the nickel producing industry |
| Description of Disease | Description of Process |
|---|---|
| Primary malignant neoplasm of the mesothelium of the pleura of peritoneum [sic] |
Any mining, milling, manufacturing, assembling, construction, repair, alteration, maintenance or demolition process involving the generation of airborne asbestos fibres |
| Primary cancer of the nasal cavities or of paranasal sinuses | Any process at the Copper Cliff sinter plant of Inco Limited |
| Primary cancer of the nasal cavities or of paranasal sinuses | Any process in the Port Colborne leaching, calcining and sintering department of Inco Limited that was practised before January 1, 1966 |
Compensation of cancers where work-relatedness is not presumed
In Ontario, as in many jurisdictions, workers diagnosed with cancer may still apply for – and be entitled to – compensation even when their cancer is not listed in a presumptive schedule or where their exposures do not correspond to the exposures stipulated under a presumption. In these cases, it must be shown, on the balance of probabilities, that their disease was contracted out of or in the course of employment by reason of their exposure to hazards in the workplace (19,20). The requirements for what must be proven vary by jurisdiction, but generally it is necessary to provide evidence that it is more probable than not that the disease was caused by the worker's employment, even if the worker was exposed to other hazards outside the workplace (19,20).
In Ontario, relevant policies are found in Chapters 11, 16 and 23 of the OPM. Ontario does not have a general policy on determining work-relatedness for occupational cancer claims. Excluding the one policy for cancers in firefighters, occupational cancers account for 12 of the 22 occupational disease policies included in these chapters. Of the 12 occupational cancer policies, 7 provide guidelines on adjudicating lung cancer claims and 2 provide guidelines on adjudicating laryngeal cancer claims. The remaining 3 occupational cancer policies provide guidelines on nasal cancer, gastrointestinal cancer, and mesothelioma. All of the WSIB’s occupational cancer policies considered in this review are listed in Appendix 2.
Footnotes
- footnote[1] Back to paragraph The term ‘burden’ refers to the human impact and economic cost associated with a cause of disease.
- footnote[2] Back to paragraph Includes submitted, as well as accepted claims.
- footnote[3] Back to paragraph The benefit of the doubt provisions are set out in Section 119 [2] of the Act and are interpreted in Policy 11-01-13.
- footnote[4] Back to paragraph The other method used is the application of sections 15.1 and 15.2 of the Act (and reference to O. Reg 253/07) to claims from firefighters. As noted elsewhere in this report, discussion of firefighter claims is outside the scope of this review
- footnote[5] Back to paragraph In claims with a diagnosis of a cancer recognized by presumption, entitlement is first determined by considering whether the worker's exposure meets the criteria set out in the second column of the appropriate schedule. If these criteria are not met, entitlement is then considered under any relevant policy or on a case-by-case basis. Case-by-case adjudication is based on the facts of the claim and an assessment of evidence of causal connection between occupational exposure and the disease.
- footnote[6] Back to paragraph Internal resources include the following: occupational and other specialist physicians, advanced practice nurses, occupational hygienists, and Operational Policy Branch support (includes policy and scientific support).
- footnote[7] Back to paragraph Ontario Regulation 253/07 also includes a list of 17 cancers that are prescribed diseases for the purposes of Section 15.1(4) of the Act.