Part 1: Introduction
There is significant diversity in Ontario’s correctional services (CS) workforce, likely consistent with other jurisdictions. The diversity is inherent in the individuals working in corrections, the employment positions, the location of services, and the differences in training, operations, and management that contribute to the complexity of the system. In Ontario, institutional and community CS provision and youth justice (YJ) is the responsibility of both the provincial and federal governments. CS provision is achieved through government-operated and service-level agreements with non-governmental organizations. This report does not specifically differentiate between provincial and federal institutions although significantly more information was provided by provincial service correctional services employees (CSE).
In Ontario, these are the categories of CS employees:
- correctional officers/youth service officers
- administrative staff
- management – all levels
- probation and parole officers/youth probation officers
- health care service providers
- other supportive/service-related staff
Public safety personnel/professionals (PSP) including CSE have a higher prevalence of suicidal behaviours over the last year of their employment as well as over their lifetime in comparison to the general population in Canada.
As PSP, CSE are often perceived differently than first responders (FR) PSP: police, fire and paramedics. The 34 deaths subject to review occurred over 15 years in the shadow of other PSP. The report is therefore titled “In the Light of Day”. The report highlights significant contributions CS professionals make while facing unique risks and challenges inherent to their occupation.
The work of a CSE is meaningful, beneficial and required in any free and just democracy. While there will always be opportunities for growth and improvement, the dedication and important work completed daily must be recognized. This is also true of the network of support for these employees, including their families and friends. Although families and friends often do not work within the field or the institutions, they are impacted by those they love and share in the hardships that are encountered. As heard during the review, these occupations have a substantial impact on employees and their families. The presence and support of a partner and children can be helpful in possibly preventing suicide. Involvement and engagement of families and friends should therefore be optimized and supported.
CSE frequently face the immediate fight, flight or freeze decision-making required to do their jobs. The requirement of split-second decisions by many CSE illustrates the importance of team unity and camaraderie to support sound judgement under the circumstances. There is a recognized risk of harm to correctional officers (CO), youth service officers (YSO), probation and parole officers (PPO), youth probation officers (YPO), healthcare as well as the other CSE from physical and emotional trauma, moral harms and/or sanctuary trauma (see below). The recognition that mental health injuries may occur is no different than a sports athlete who may encounter the daily risk of physical injury. The CSE, however, generally suffer these injuries in the shadows without the public and organizational supports afforded to others including sports figures or most other PSP/FR. For example, athletes in sports have been supported by the approach to concussion prevention and treatment which is now quite well established. Currently processes are being developed within CS to similarly respond to mental health injuries. The specifics of assessment and support provision to CSE is unique in many aspects when compared to other PSP/FR.
Throughout the review it was clear that CSE face several challenges and often internalize stress which contributes to feelings of isolation, mental health injury and other harms. To help diminish and potentially prevent these challenges, CSE should be provided with strategies to recognize and convey their experiences through training by incorporating the language of mental health and understanding occupational stress injuries. Otherwise, the individual, with their often-invisible struggles, may be further impacted with secondary effects on co-workers, family and friends.
Understanding the risks encountered by CSE and the potential impact on the health and well-being of these employees is paramount. The role of supportive and broad-based approaches to well-being that is inclusive of physical, mental, social, economic, moral, and spiritual health is required. The diversity of positions within corrections, their locations, and the varying cultures of different workplaces is too broad to be fully explored in this report, but some key points learned during this review were incorporated.
The importance of structural change, which in turn requires a work-culture growth cycle is indicative that there is no “silver bullet” approach that will immediately improve every CSE’s work environment. This process may take several years. Part of the work-culture changes required is to encourage and facilitate societal perceptional changes. As an example, during the COVID-19 pandemic how many supportive rallies occurred recognizing the dedicated and hard work of CSE tasked with maintaining the health and well-being of justice-involved persons?
CSEs face exposures to verbally and/or physically violent behaviours, directly and/or through the review of reports. Some staff respond to health emergencies such as substance-related death, and others review, educate, and at times reprimand those involved in these processes (both worker and justice-involved persons). During the review it was clear that each facility, unit and even shift has its own culture and level of complexity.
PSP have been reported to have other concurrent health issues including, challenges with chronic pain and/or symptoms of a mental health-related disorder. PSP individuals with known chronic pain were found to more likely screen positive for post-traumatic stress disorder (PTSD), depression, anxiety and alcohol use disorders. In this review of 34 deaths the following conditions were noted to be present in several individuals: depression, anxiety, PTSD, personality disorders, chronic pain, as well as alcohol and substance use disorder (see Table 2 below).
PSP have reported a higher lifetime prevalence of suicidality when compared to the general population, with men, older and/or married PSP less likely to report suicidality. The average age at the time of the 34 deaths by suicide reviewed was 50 with most individuals being defined as male. CSE and paramedics have been found to have higher odds of suicidal behaviour when compared to municipal or provincial police officers. This highlights the variable risks and differences within the PSP/FR population potentially associated with daily experiences during their work.
There have been many reports on the importance of correctional service settings to incorporate the principles of human rights and the necessity of adequate health services for justice-involved persons (WHO/UN). However, it is also necessary to stress the importance of the health and well-being of the staff who work within correctional services. Both staff and justice-involved persons share common ground, as they co-exist in the institutional environment and often come from the same communities and social backgrounds.
The Norway prison system has an approach that could be beneficial in assisting all correctional management staff and unions in management-staff approaches to improve CSE wellbeing. The four guiding principles from the Norway system were developed in response to CSE deaths (murdered on duty) in the 1990s:
- Equality: Treatment of all individuals, staff and justice-involved persons, predicated on equal rights and access to services except the limitation to freedom of movement (for those in closed custody). Those in closed custody could earn potential, after a certain timeframe, time-limited releases. If all are treated equally and accept that all people are capable of errors in decision-making, they could all live in the same community which benefits everyone.
- Human dignity: This exists for all those involved in corrections, CSE as well as justice-involved persons. It is hard for people treating other individuals that are not afforded similar levels of equality and dignity to not be impacted personally over time.
- Normality: Function within a normalized environment similar to society. This would help limit the potential for moral injuries to staff. Time to process events at work prior to getting home for staff so as not bring “work” home would be beneficial.
- Rehabilitation: This should be predicated on the belief that people can change, and correctional institutions are working to re-integrate individuals into their respective communities.
Learnings from the review demonstrate that staff experience variable degrees of isolation depending on their job, stricter rules and regimens related to operating procedures, hierarchical structure, team dynamics, bureaucracy, and the degree of control. In addition, society’s perception of those working within corrections is often not as positive when compared with other PSP.
Working in correctional institutions presents both physical and non-physical challenges. Several participants spoke about overcrowding in the institutions, outdated buildings, and the physical and emotional harms associated with interacting with justice-involved persons. Some contributors also reported co-worker interactions as significant challenges. Exposure to morally injurious events (discussed below) was frequently cited by most participants in this report. They detailed an unpredictable environment of high demands and accountability with limited personal control which has been shown to impact the well-being of CSE.
Challenges and risks are faced by the CSE over different life cycles of their employment. Life cycles of their employment, as outlined in the report, included the following stages:
- pre-placement/interview and assessment stage
- early years of employment (first two years)
- experienced employee (after two years)
- on leave: medical, administrative, or other
- retirement, resignation and post-retirement
Many of the recommendations were categorized with the specific life-cycle stage of the employee.
Workplace culture was impacted by one or more of the following:
- Management-staff: management-led related processes, policies and behaviour-modelling to ensure a healthy workplace. This was noted by most who commented on these approaches as the most impactful for organizational wellness. How leaders were selected, trained and supported was noted to potentially be the most helpful in this category.
- Staff-management: staff-specific activities that ensure their wellness and contribute to organizational resilience. Adherence to the assigned number of hours worked, shifts that support proper sleep hygiene, and other health-enhancing behaviours were advocated by most participants.
- Staff-staff: all staff-related supports and service provision for each other (at various levels). Peer-support processes, formal or informal, are included in this area.
The presence of a “toxic/traditional masculinity” culture and the potential co-existing emotional repression and need to just cope/manage, self-reliance and risk-taking in PSP/FR was discussed by many participants. The level of toxicity leading to lack of support, shame and blame behaviours, and feelings of isolation by individual CSE was described as ongoing, concurrent with the daily hazards inherent to the specific work environment. It was suggested that system-related approaches to prison reform related changes in the justice system are necessary for staff wellness.
CSE, as a subset of PSP, are known to be at risk for and/or impacted by many events that adversely affect their health and well-being. Given the unique risk and stigma for Indigenous, Black, racialized and 2SLGBTQIA+ staff, the importance of gender and racially inclusive language, service provision, and sensitivity training along with the removal of any barriers to care, as required, should be addressed in conjunction with the appropriate available resources.
A. Review of findings of 34 deaths by suicide of correctional service employees
The Office of the Chief Coroner of Ontario/Ontario Forensic Pathology Service (OCC/OFPS) case management systems were searched for deaths by suicide of persons who either worked as a CSE, were on leave from their position, or retired from a CSE position. Information obtained from the investigations into these deaths was shared in a deidentified manner with all the employer/employee-related staff, service providers, researchers, union-related individuals, provincial and government service providers and other CSE-related experts during this review. The categories of CSE applied during the review were:
- correctional officers/youth service officers
- administrative staff
- management – various levels
- probation and parole officers/youth probation officers
- health care service providers
- other supportive/service-related staff
34 CSE deaths by suicide investigated by our office included:
2010-2019 – 17 deaths reviewed (10-year period)
- 13 men
- 4 women
2020-2024 – 17 deaths reviewed (five-year period)
- 14 men
- 3 women
The review was informed by analysis of de-identified aggregate data from the 34 deaths, in depth individual reviews were not completed. The average age of those who died was 50 for both time periods as well as for men and women.
(Note: there are likely additional deceased persons that were not included in our review because their occupation was not documented or there was an undetermined conclusion from their death investigation.)
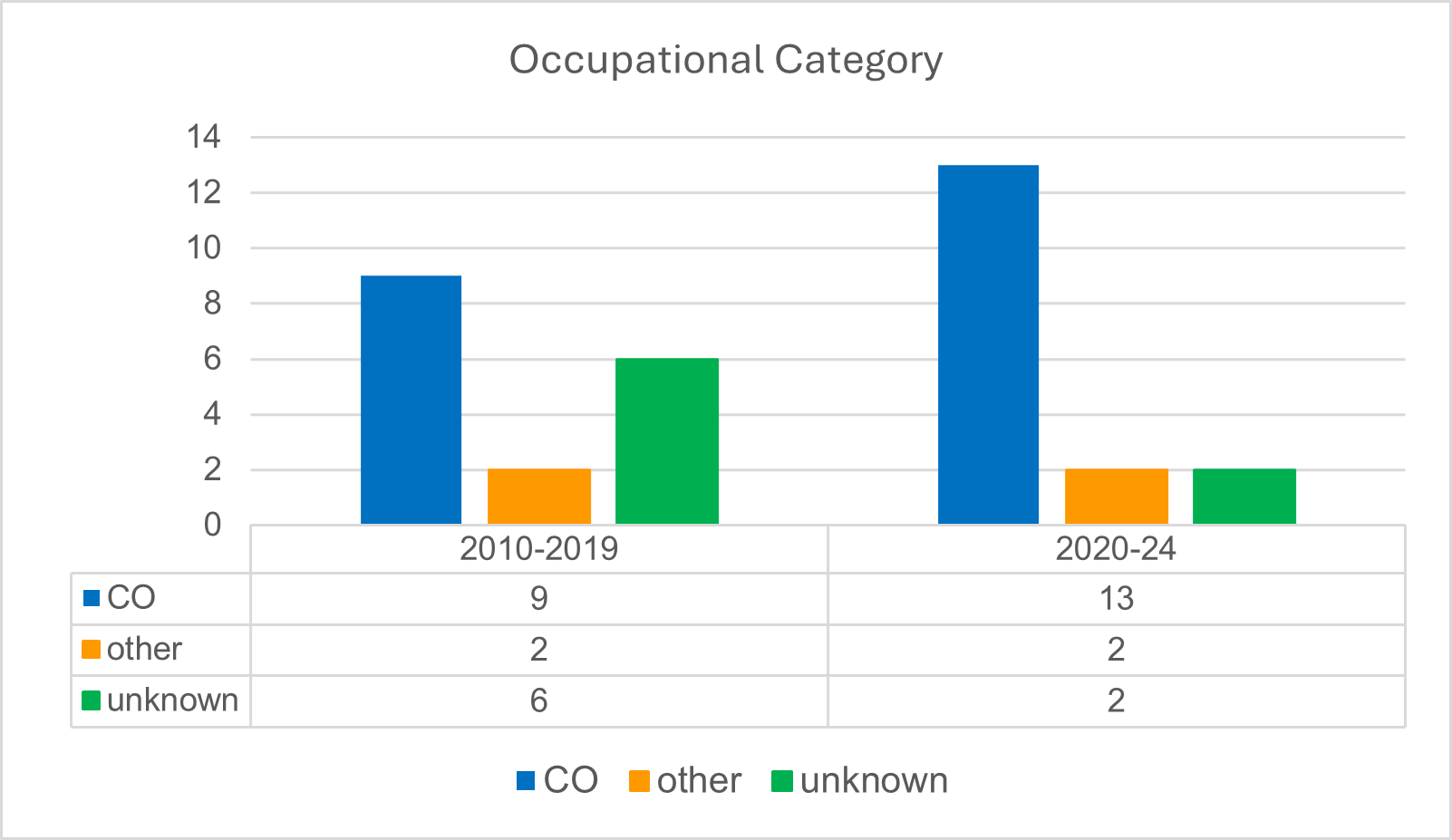
CO comprised the majority of suicide deaths within CS for both timeframes, although several death investigations did not document the specific CSE position (6 between 2010-2019 and 2 between 2020-2024). This data may be impacted as specific documentation of the specific position with corrections by the coroner may not have been accurate. Figure 1 summarizes these findings:
Figure 1: Occupational category as CO vs. other of CSE who died by suicide
The documented presence of a note at the scene or a message on the deceased person’s phone is shown in figure 2 below (4 cases between 2010-2019 and 1 case between 2020-2024 did not document their presence or absence).
Figure 2: Number of CSE with a reported previous suicide attempt as well as a “note” left at the scene or on the deceased person’s phone
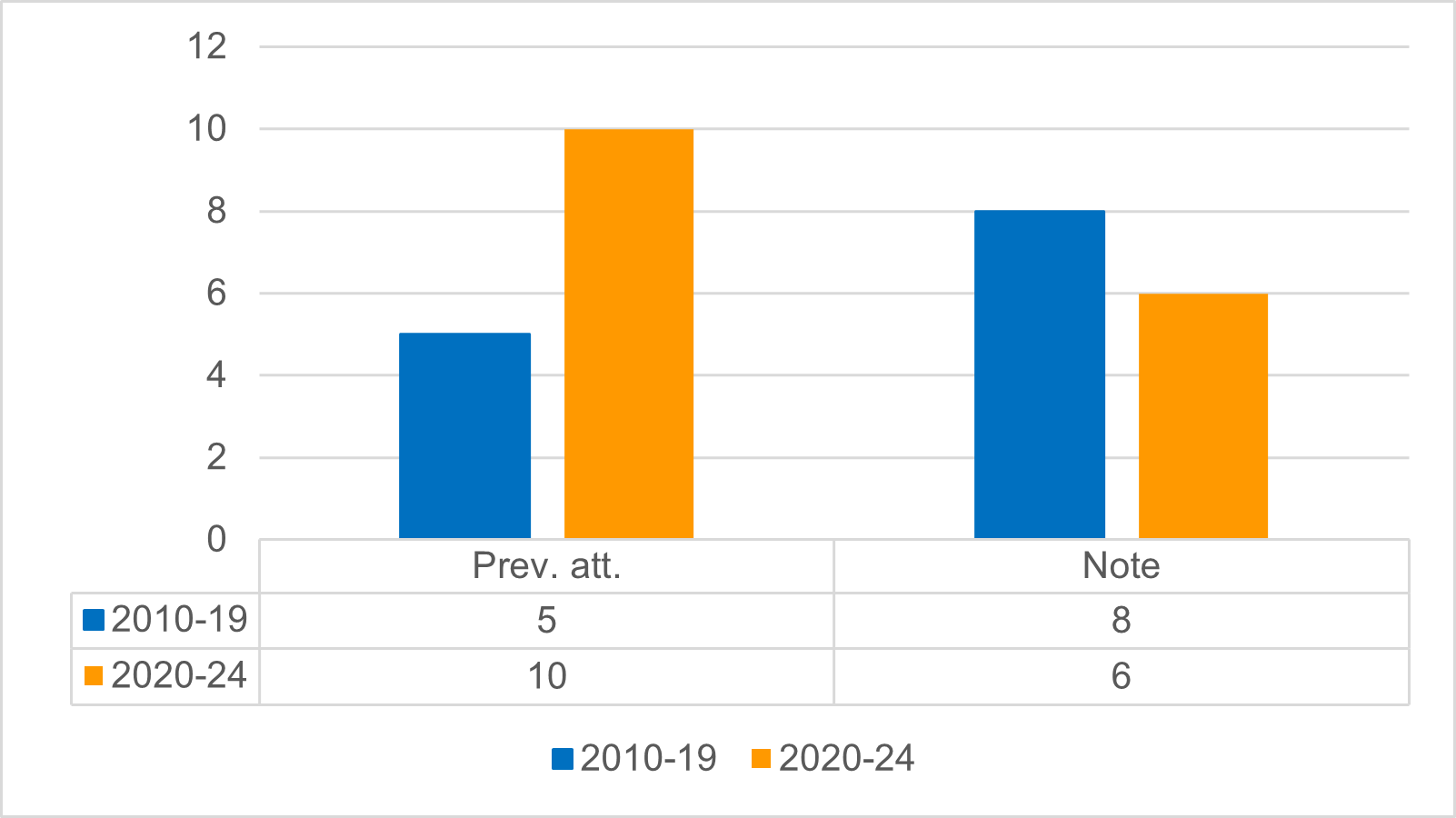
Table 1 provides the cause of death categories for the 34 individuals. To ensure confidentiality, when a category included less than 5, it was represented by the <5 (there were between 1-4 deaths included).
| Cause of death | 2010-2019 | 2020-2024 |
|---|---|---|
| Firearm-related | <5 | 7 |
| Hanging/ligature-related | 6 | 6 |
| Sharp force injury (knife-related) | <5 | <5 |
| Drowning (bathtub, pool, body of water) | <5 | <5 |
| Alcohol/drug toxicity | 5 | <5 |
| Burn-related | <5 | 0 |
| Blunt-force trauma (fall/motor vehicle collision) | <5 | 0 |
Table 2 summarizes the presence of co-morbid health conditions, and mental health conditions. Note: the duration of diagnoses and treatments was not available.
| Part mental health conditions | 2010-2019 | 2020-2024 |
|---|---|---|
| Major depressive disorder | 10 | 10 |
| Anxiety | 2 | 3 |
| PTSD | 2 | 5 |
| Personality disorder | 0 | 2 |
| Schizophrenia/bipolar disorder | 1 | 2 |
| Alcohol/substance use disorder | 3 | 5 |
| Disability (at time of death/prior) | 2 | 4 |
| History of chronic pain | 2 | 2 |
| Recent mental health admission | 3 | 4 |
Coexistent issues included in both work and non-work-related factors were:
Work specific factors:
- previous PSP related job (often policing/military)
- job loss/absence or disability-related leave
- work-related transfers
- exposure to traumatic situation (physical assault or witness-related trauma)
- work-related testifying in court proceeding or inquest.
- stigma or other impact of public/press perceptions on workforce/institution
External (non-work) factors:
- marital/relationship separation/significant relationship discord
- personal or interpersonal distressing events
- personal moves
- retirement from CSE
- personal loss of parent, spouse, sibling, child and/or another significant person
- police involvement/charges not work-related
B. Moral injury
In a 2024 report by Ricciardelli et al. both moral distress and moral injury within corrections workers was reviewed. Researchers have described how moral distress (although not formally in the Diagnostic and Statistical Manual of Mental Disorders -DSM-5-TR-for psychiatry, it is referenced in the latest version as “psychological unease”) arises when an individual is required to act within their institution of employment that is not aligned with their personal ethical and/or moral framework. Moral distress can become injurious to those who participate in, or are unable to prevent actions that violate their own moral beliefs and/or those who experience betrayal by a legitimate authority in a high risk setting. Witnessing or being exposed (directly or indirectly) to workplace violence, death, overcrowding in small cells, are some of the situations that are experienced by CSE. The impact of institutional practices/policies and discourse is recognized as a contributor to potential moral injuries/harms. The Ricciardelli study found three domains of possible moral harm for CO working in a correctional institution:
- Rehabilitation: CO may have concerns about the amount of rehabilitation provided to those in their care, if any has occurred, its effectiveness and impact.
- Societal protection: CO impacted by overcrowding, impact of justice system in terms of support for justice-involved persons as those who are also in need of protection.
- Punishment: CO employees are not supposed to judge but given they recognize the difficult living conditions that exist, provide safety in a difficult environment, as well as being aware of the limited consequences for behaviours within the institution (such as acts of violence) that would not be acceptable in any non-custodial environment.
Injury can occur from the ongoing impact of all these events when the presence is not recognized, or there is no treatment or management to mitigate the impact of the associated distress. Moral injury could result in one (or more) of the following:
- PTSD
- addictions – alcohol, substance use disorder, other addictive behaviours
- social impact– interpersonal conflicts, spiritual/cultural impact
- mood/anxiety disorders
Table 2 (above) documented the presence of these four issues in the 34 individuals reviewed.
In a recent study by Ricciardelli et al. looking at the mental health and occupational experiences of management in institutions there was a high prevalence of these mental health disorders (56%) with one-third of the participants having reported previous suicidal ideation. The study noted that many did not seek support services indicating that there should be work done to enhance this in the work environment.
Results from a 2017-18 Occupational Stress Employee Survey of Ontario CSE illustrated reported challenges.
- 7% suicidal ideation in the previous year vs. 2.5% for general population
- 2.6% previous year suicidal planning
- 26.6% lifetime suicidal ideation vs. 11.8% for general population
- 11.9% lifetime suicidal planning vs. 4% for general population
| Type of disorder | All staff | Correctional officers | Probational officers | Administration |
|---|---|---|---|---|
| Screened positive for at least one mental disorder | 58.2% | 59% | 63.2% | 52% |
| Major depressive disorder | 37% | 39.7% | 37.4% | 40% |
| Generalized anxiety disorder | 30.5% | 32% | 33.1% | 23.3% |
| Post‑traumatic stress disorder | 30.7% | 34.2% | 25.5% | 30% |
Each of these disorders/challenges present with a variety of signs and symptoms that if detected at earlier stages could allow earlier intervention to reduce progression or severity. Several of the recommendations that were developed inform efforts to prevent or limit morbidity.
The following considerations relate to the recognition and/or reduction of the impact of moral injury and other harms informing some of the recommendations:
- Informing staff working in any CS positions the language of mental health risks, their early recognition and management, and concerning signs and symptoms. This would provide everyone with baseline tools to ensure their own well-being while also being aware of how to potentially recognize, describe and provide assistance to their co-workers.
- Informing staff and society about nature, origin, and impact of moral distress and injury as well as early recognition and treatment.
- Importance of understanding roles and boundaries of staff and others in education, symptom and risk recognition, resource provision and institutional supports.
- Societal supports and understanding to ensure appropriate protection and understanding of CSE and need for the required treatment interventions.
- Treatment of social/medical complications inclusive of appropriately trained clinical professionals, social support provision to employees and their families/friends, and programs to educate and enhance growth after any type of trauma (mental, social, moral, physical, other) and skill development/enhancement to manage these experiences.
- Ongoing research as more data becomes available on these processes. This is inclusive of postvention programs and supports if an employee’s death is a death by suicide.
The importance of these considerations has been reported within the context of public safety professions, such as CSE, that reiterates the need for early detection and management of conditions impacting physical and mental health as well as addictions management. Reported suicide rates of PSP increased in the USA from 2001-2021 and that a majority of individual deaths by suicide occur on their first attempt (79%) reinforcing the importance of early detection and treatment. During the review the ongoing cycle of work-related stress due to the daily exposure to traumatic and morally injurious events with the genesis and perpetuation of addiction-related behaviours was reported.
The inclusion of moral injury as a factor in mental health diagnoses in the most recent DSM manual may help ensure treatment-related approaches are more sensitized to its impact and need for management.
A survey of CSE in Newfoundland and Labrador illustrated a concerning prevalence of a variety of conditions.
- Almost 50% of those surveyed screened positive for one or more of PTSD, depression, anxiety and or alcohol use disorder
- Those surveyed reported at least one “potentially psychologically traumatic event” (PPTEs):
- exposure to physical assaults (87.2%) including with a weapon (78.6%)
- exposure to sudden death due to violence (85.7%)
- exposure to accidental death (77.4%)
- exposure to abusive language, mental health crises (both >90%)
- feeling unsafe/insecure in workplace
- having mental health challenges impact them on daily basis
Also, in a Ricciardelli et al report related to provincial and territorial CSE reported:
- 58% of CSE screened had at least one mental health disorder with major depressive disorder the most common.
- the prevalence varied amongst the provinces and territories with highest risk in CO.
It was evident from the research, review participants, moral injury experts, current/previous CSE, and their supports that PPTE are significantly present in the day-to-day operations of corrections.
The importance of leadership support was noted as a strong predictor of CSE health assisting with limiting and preventing the impact of moral injury in the workplace. Simply stated the importance of being heard, understood, and valued would go a long way in health maintenance and illness prevention. In contrast the perception of betrayal by co-workers and management was reported by many of the families who participated in this review.
C. Sanctuary trauma
Sanctuary trauma, as defined by Dr. Steven Silver, refers to the trauma that “occurs when an individual who suffered a severe stressor next encounters what was expected to be a supportive and protective environment and discovers only more trauma.” Sanctuary trauma experienced by CSE was described by review participants especially during incident reviews when seeking help and/or support. It was reported that there is an expectation that CSE be able to manage/handle all the situations they face and “just do the job.” The increased scrutiny, complaints, and challenging communications from the public to CSE staff may be contributing to this kind of trauma. The importance of an incident analysis and response framework generated within trauma-informed principles was recognized, suggesting benefits of modifying approaches to managing accidents or adverse events.
D. Protective factors
Potential protective factors and processes identified during the review include:
- Comprehensive, trauma-informed employment practices beginning with hiring and extending through to retirement that support recognition, occupational advancement, peer support, mentoring, as well as continuing education and implementing best practices.
- Clear, comprehensive workplace guidelines and training materials for incident reviews, safety-related processes, educational opportunities, hazard identification and other related management processes.
- Supports through all life cycles of employment that inform and educate staff regarding their ability to: identify and monitor issues early, seek appropriate and timely treatment resources, and recover and return to work (as necessary/applicable). An example of this is Wounded Warriors Canada’s Trauma Resiliency Training (train-the-trainer), which was first adopted by Correctional Services Canada at Collin’s Bay, Millhaven and Bath Institutions and will be available at all federal and provincial institutions in 2026.
- Those suffering from addiction-related behaviours associated with or exacerbated by their employment in CS such as alcohol and drugs, gambling, exercise, and/or sex-related addictions, should have ability to access confidential, appropriate and timely treatment options. Current options have been reported to have limited accessibility.
- Modelling appropriate behaviour, having appropriate and available personal supports with a trained co-worker, and availability of supportive and trained management staff in the various work locations that maintain confidentiality. This was often stated to be most effective when embedded in the Management-Staff processes.
- Work environments that strengthen supportive team interactions, educational programming for work and private life (health, financial, and other social supportive programs such as addiction-related supports).
- Work environments and processes supportive of a healthy workplace in terms of holistic wellness to ensure quality of work and life inclusive of physical, social, financial, social and cultural well-being.
- Internal and external recognition that those that work in CS are good, caring people who are providing a necessary service that benefits society.
At a House of Commons Standing Committee on Health hearing on May 16, 2017, Dr. J. Sareen stated that risk factors for PTSD and depression included: childhood trauma exposures, fewer social supports, female, poverty, and physical assaults/injuries/TBI (traumatic brain injury). Protective factors reported by Dr. Sareen include the presence of social supports, higher levels of training/education and stronger connections/networks in the community. The review participants reported that presence of described risk factors may be further stigmatizing for CSE. The reluctance to seek help or support arises from concern of possible repercussions preventing early intervention. Several participants referred to a common saying that “there is no crying in corrections” as a part of a “toxic masculinity” culture that can occur in correctional settings. The perception that vulnerabilities are weaknesses requires reframing to recognition that these may be a sign of a need for support.
Another frequently referenced resource is the Department of the Air Force “Total Force DAF Standardized Suicide Fatality Analysis” released in 2023. This report highlights four major categories that contributed to the suicide risk of its members: Societal, Organizational, Relational (similar to between staff and between individual CSE and non-CSE persons), and Individual (mental/physical health, sleep, addiction, other). These categories highlight the importance of management-staff; staff-management and staff-staff approaches and their respective potential impacts.
The importance of live, in-person training and onboarding was recognized by many that participated in the review. The exposure to in-person training to experience the “sights, sounds and smell of the environment” was considered an important process along with the development of social supports and networks amongst the trainees. It was suggested that virtual, self-completed, training may be a barrier to fully understanding the “real human” aspects of the job(s). The importance of this has been recognized with the introduction of on-site CO training in the institutions. This approach provides the opportunity to tour work locations as part of on-site training and can help de-mystify some of the perceptions that new hires may have prior to their employment.
The review recognized the benefit of providing all employees with training on managing daily stress-related events with the use of physical maneuvers, such as breathing-related exercises concurrent with their response-related skillset (such as use of force training). The importance of training in crisis management has been reported as well as the importance in shifting away from permissive attitudes towards suicide to seeing it as an “unjustified behaviour”.
Inherent to successful training is the requirement that those working in a corrections environment have the education to identify signs of distress in themselves and co-workers. The educational and skills training should be inclusive of the employee’s families or friends as identified by the employee. Health-seeking by employees should be normalized and supported with further requirement for trusted care to be provided by those with correction-specific knowledge and experience. The comprehensive involvement of the employee with an informed circle of care would likely contribute to healthier outcomes.
The management of adverse events or errors that may occur while working was an area of challenge recognized during the review. The review found that a culture of openness for identification and exploration of errors, with a goal of improvement and error-prevention, was lacking. Concern was identified regarding an over-riding culture of critical analysis leading to consequences vs. recognition of the contribution of environmental and other factors. The perceived predisposition to error-identification and blaming vs. that of recognition of those working in challenging situations making difficult decisions was frequently stated. There was no dispute about the importance of documenting and managing situations that require disciplinary processes. The existence and promotion of an environment of kindness from the first day of training throughout employment was recognized by many as a meaningful goal for CSE. This can, and often does occur, with the provision of open, direct and non-judgmental communication, incident analysis and the learning that results from this analysis.
Attending to the psychological safety of criminal justice system workers has been studied and the importance of dealing with stigma, enhancing health-seeking behaviours, preparing employees for potentially traumatic incidents within the context of culturally informed methods described. This study indicated that working toward improved physical health and lifestyle, peer support, improved working conditions and safety were important.
The review recognized that personal privacy was a significant consideration. CSE reportedly often do not reach out to organizational supports, such as WSIB, because they fear the information will be shared with management or that their co-workers will become aware. They believe that seeking help will have an impact on how they are perceived. This is especially true in smaller locations and communities where challenges regarding anonymity may occur. The need for regular training, mental health related assessments by appropriate professional, confidentiality and enhanced workplace morale and collegiality has previously been documented for CSE in Ontario and is reflected in the recommendations.
The Canadian Centre for Occupational Health and Safety (CCOHS) designed an approach to occupational hazard reduction to hazardous materials, the Hazard and Risk – Hierarchy of Controls. Its main categories may be applicable as an approach for CS to reduce hazards for CSE. The categories are ranked in descending order of effectiveness:
- Elimination: removal of the specific risk
- Substitution: replacing the specific risk with a lower risk (similar to harm reduction principles)
- Engineering controls: specific controls utilized when the risk occurs to minimize impact (such as debrief, crisis interventions)
- Administrative controls: work systems established to assist in prevention of as many risks as possible
- Personal protective equipment (PPE): although PPE is generally specific to physical protection it could be considered to include specific physical and emotional barriers to limit/prevent exposure of CSE to the various harms to which they are exposed
Awareness of these controls in the reduction of hazards in the CSE workplace may be helpful. The CCOHS also has information regarding psychological health and safety related to many of the issues recognized in the review related to the workplace.
E. Current services provided for correctional service employees
1. Employee Family and Assistance Program
The main mental health support program offered by the Ontario Public Service (OPS) for employees and eligible dependents, is the Employee Family and Assistance Program (EFAP). Through external providers, EFAP includes resources, counselling and programs. Several review participants indicated that while having around the clock availability is helpful, the counsellors often have limited skills and experience to address the specific challenges and conditions faced by CSE. CSE often found themselves providing details and clarifying information about their work conditions that was potentially traumatizing to the EFAP support person. This contributes to CSE reluctance to contact EFAP for support, especially for work-related concerns and/or issues.
Concerns were raised regarding confidentiality of EFAP and whether workplaces would be informed that EFAP was contacted. Challenges were experienced navigating the system of EFAP, adding an additional perceived barrier accessing the services. From providing intake information to having a support person assigned was reported to not be consistently managed. This was noted as a barrier for some CSE to follow through on accessing these services.
2. Peer support services
Peer support services are provided both internally as well as with external service providers. Benefits of peer-related experiential sharing include being understood and supported as well as helping resolve feelings of isolation. Challenges that these programs could address included:
- confidentiality concerns regarding the interactions and potential of management being informed
- CSE organizational mistrust and how shared information could impact the reporting employee and co-worker perception
- ensuring the peer support team is staffed by the right individuals possibly nominated for these positions by their peers
The provision of a critical incident stress management (CISM) is led by a person with a clinically appropriate background has been reported to be beneficial in increasing opportunity for trauma-informed supports being provided in an institutional setting for events such as a CSE-related death by suicide. CISM-related individuals would travel to the location of defined events that require management and debriefing. This has been noted to be beneficial in increasing the opportunity that trauma-informed supports are being provided in an institutional setting for events such as a CSE-related death by suicide. Some of the potential incidents that CISM could respond to include deaths in custody, assault of staff, and riots. It was reported by some participants that facility staff were likely to be referred, while community CSE staff (probation/parole) were more likely to self-refer. The use of a CISM approach that is predicated on provision of assistance and stabilization while also obtaining information regarding the event could help ensure the psychological safety of the CSE. This is available within the federal correctional system and the MCCSS/YJD. Provincial adult institutions have moved to a peer-support system.
3. Training
A number of initiatives have been provided in correctional services over recent years, including safeTALK (training for staff to gain knowledge in the identification and providing assistance to those considering suicide), BOS (Before Operational Stress – to help PSP manage operational stress) and ASIST (Applied Suicide Intervention Skills Training). SOLGEN has implemented safeTALK and will be implementing an eight-week mandatory BOS training course that will begin next year (2026) as well as ASIST and other programs. Joint tables involving union and management, provincially and federally, have assisted in delivering educational programs and services to CSE. The importance of management modelling support of culture change was recognized.
Table 4: SOLGEN Corrections Employee Wellness Training Framework
New recruits
Before Operational Stress
virtual, 8 hours
All CSE (management & bargaining)
Trauma Resiliency Training
in-person, 90 minutes (mandatory training)
Stress Resilience Training System
virtual, 20 hours
Employee Suicide Prevention Initiative (ESPI): safeTALK
in-person, 3 hours (mandatory training)
ESPI: Applied Suicide Intervention Skills Training
for future training
Mindfulness-Based Wellness & Resiliency Program
virtual, 11 hours
in-person, 32 hours to 72 hours
Management
Manager Mental Health Leadership Certificate Pathway
in-person, 1 week
Workplace Mental Health Leadership Certificate Program
in-person, 14.5 hours