2023 Medical Assistance in Dying (MAiD) Review Team Annual Report
Read the committee’s 2023 annual report on medical assistance in dying (MAiD) deaths in Ontario.
Introduction
Acknowledgment
We wish to acknowledge the individuals represented in the information provided and the losses experienced by their families, loved ones, and communities. We hope that by presenting this information, we can support continued improvement in how MAiD is provided in the province of Ontario.
Purpose
All data presented in this report were submitted to the Office of the Chief Coroner (OCC) by MAiD practitioners as required for Health Canada mandatory reporting and are Ontario-specific. All data are reviewed to ensure accuracy and completeness. The purpose of this document is to share the activities of the MAiD Review Team (MRT) in the oversight for MAiD as part of the OCC. Additionally, this report will illustrate the data collected and provide a summary of MAiD practice within Ontario. Additional context is provided where available to expand on the findings. We extend our thanks to all the providers who take the time and care to complete the necessary documentation and provide the level of detail necessary to support OCC oversight.
Definitions
- MAiD Practitioner:
- a medical or nurse practitioner who has knowledge of and participates in providing access to Medical Assistance in Dying (MAiD) within Ontario.
- MAiD Provider:
- a medical or nurse practitioner who administers or prescribes a lethal medication to cause death.
- MAiD Assessor:
- a medical or nurse practitioner who provided a written opinion confirming that the person met eligibility criteria (i.e., includes both the MAiD provider and secondary assessor).
Oversight for MAiD at OCC
Federal MAiD legislation, Bill C-14, enacted in 2016 included regulations for the Minister of Health to develop a monitoring process for data collection to promote insight and transparency into how the legislation was working. “Regulations for the Monitoring of MAiD” was enacted in 2018 and set out the mandatory data required for submission by practitioners who receive a request for MAiD and pharmacists who dispense the drugs.
Provincial legislation passed in 2017 (Bill 84) changed how MAiD would be managed in Ontario. The Bill updated the Coroners Act to require all MAiD deaths to be reported to the Office of the Chief Coroner (OCC), and any associated documentation requested by a coroner for the review of that death was to be provided to determine the need for investigation.
Through an agreement between the federal government, Ontario Ministry of Health and the OCC, the OCC became the designated recipient for Health Canada data. Ontario developed a hybrid reporting system in which all MAiD deaths are reported to the OCC and all other outcomes following a MAiD request are reported directly to Health Canada by the MAiD practitioner. Following these legislative changes, the OCC established the MAiD Review Team (MRT) to provide a consistent approach to oversight, review, and data gathering for MAiD.
Further federal legislative changes occurred in 2021 with Bill C-7 and as a result, changes were made to the mandatory reporting requirement which expanded the data to be collected. “Regulations Amending the Regulations for the Monitoring of Medical Assistance in Dying” came into force on January 1, 2023.
MAiD Review Team (MRT)
The MRT is composed of a group of highly skilled registered nurses (RNs) with various health care experiences and backgrounds to inform MAiD death review to determine compliance with the legislation, evaluate care concerns and inform MAiD practice improvements. The MRT are knowledgeable of and follow death investigation processes. The MRT RNs are appointed by the Chief Coroner under the authority of the Coroners Act to exercise the investigative powers and duties of a coroner or the powers of a coroner under subsection 15 (1.1).
In the time since MAiD became legal the approach to MRT review has progressively changed. Initially all MAiD Practitioners were required to directly contact the OCC immediately following the death to speak with a member of the MRT who would gather information to determine the need for investigation. The MRT would next review submitted records to capture the required data for Health Canada reporting on behalf of the provider. With the progressive increase in the number of individuals accessing MAiD, most of which did not proceed to investigation, the OCC embarked on a modernization initiative in February 2022 to streamline and improve the review process leveraging technology with the further goal of improving the quality of data gathered. This initiative allows for greater focus on the cases that have increased complexity and carry greater risk of legislative concerns which could inform learning and spawn recommendations that could help to improve MAiD practice.
As of January 1, 2023, all MAiD deaths are reported to the OCC through an electronic form submission (the MAiD Death Report (MDR)) that facilitates submission of all data required to meet the Health Canada mandatory reporting in addition to data required to determine the need for further review or investigation of a death. Every MDR is reviewed by a member of the MRT for completeness and accuracy. Any gaps are followed up on for clarification. A representative of the deceased person is directly contacted by a member of the MRT following the death to inquire about any issues or concerns that may have arisen during the assessments or provision. If any issues or concerns are identified, additional records are requested for review, or an investigation is completed to evaluate the circumstances surrounding the issue to identify if any recommendations that could arise can be shared with the MAiD provider or the broader MAiD community.
Mission and values
The MRT developed this Mission Statement:
The MAiD Review Team works within the Ontario Office of the Chief Coroner to employ our diverse range of clinical experiences and expert knowledge of MAiD legislation to provide independent review and legislative oversight of MAiD practice to ensure public safety.
Our values are: Public Safety, Collaboration, Empathy
- The MRT established the following mandates:
- The MAiD Review Team leads the field in providing comprehensive monitoring and review of legislative and regulatory compliance for each MAiD death that occurs in Ontario.
- The MAiD Review Team engages with stakeholders, practitioners, and families with respect, compassion, and empathy to ensure that every Ontarian had access to a dignified MAiD death after receiving high-quality care.
- The MAiD Review Team interacts with clinicians, communities, and regulatory, professional, and government organizations to promote exemplary MAiD practice through knowledge translation and public transparency of the MAiD review process.
MAiD Death Review Committee (MDR)
With the expansion of MAiD legislation in March 2021 to include non-reasonably foreseeable natural deaths (NRFND) and the introduction of the waiver of final consent for reasonably foreseeable natural deaths (RFND), MAiD requests and the conditions for which people sought a medically assisted death became more complex. The MAiD Death Review Committee (MDR) was developed to support the work of the OCC in the oversight of MAiD deaths in the province of Ontario. The first committee meeting was held in January 2024.
The committee is comprised of 16 members from across multiple disciplines (law, ethics, medicine, psychiatry, social work, nursing, and a member of the public) who bring a diverse background of expertise in providing advisory support to the coroner’s death investigation system.
The MDR seeks to provide recommendations and guidance that can improve the practice of MAiD through the evaluation and discussion of themes identified by the MRT through the review process as well as the oversight of MAiD.
Reporting on the activities and recommendations from the MDR is planned and is not included in this report.
2023 Data MAiD review statistics
All MAiD deaths submitted to the OCC are reviewed by a member of the MAiD Review Team (MRT). In 2023, there were 4,644 MAiD deaths. The information presented is based on 2023 information that was captured following submission of MAiD Death Reports (MDR).
Case breakdown
While a natural disease, illness, or disability is associated with the majority of MAiD deaths, at times some circumstances may lead to a request for MAiD that may not be considered natural in nature. In Ontario the underlying condition that prompted the request for MAiD is provided as the cause of death on the medical certificate of death. In 2023, 97.5% of all MAiD deaths were natural in manner, with 2.5% due to non-natural manners of death following investigation.
Cases investigated
All MDRs submitted to the OCC are individually reviewed to determine the need for further evaluation or investigation. As per the Coroners Act, any death where there is the potential for non-natural involvement must be reported to a coroner for investigation and to determine the manner of death (natural, accident, suicide, homicide, undetermined). In addition, investigation may occur in deaths with care concerns, potential practice deviations, legislative concerns, or family/next of kin concerns raised with, or identified by, the MRT.
In 2023, no concerns were identified in 3,861 MAiD deaths reported to the OCC. Investigation by MAiD coroner investigators was required in 271 deaths, due to factors associated with the death that contributed to a potentially non-natural involvement (fall, injury, fracture, etc.) or family or care concerns identified through the review process that required additional follow up or recommendations.
The MRT completed further review on 512 deaths which included deaths that were dual/joint provisions, when frailty or dementia was provided as the cause of death, identified capacity concerns, care or provision concerns, family concerns, Track 2/NRFND cases, or self-administration. Of these deaths, 44 deaths were further investigated after the MRT identified additional concerns. In total, 315 MAiD deaths were investigated by a coroner investigator following the initial MRT review.
The most common reason for initiating an investigation was due to an accident or injury involvement (49%).
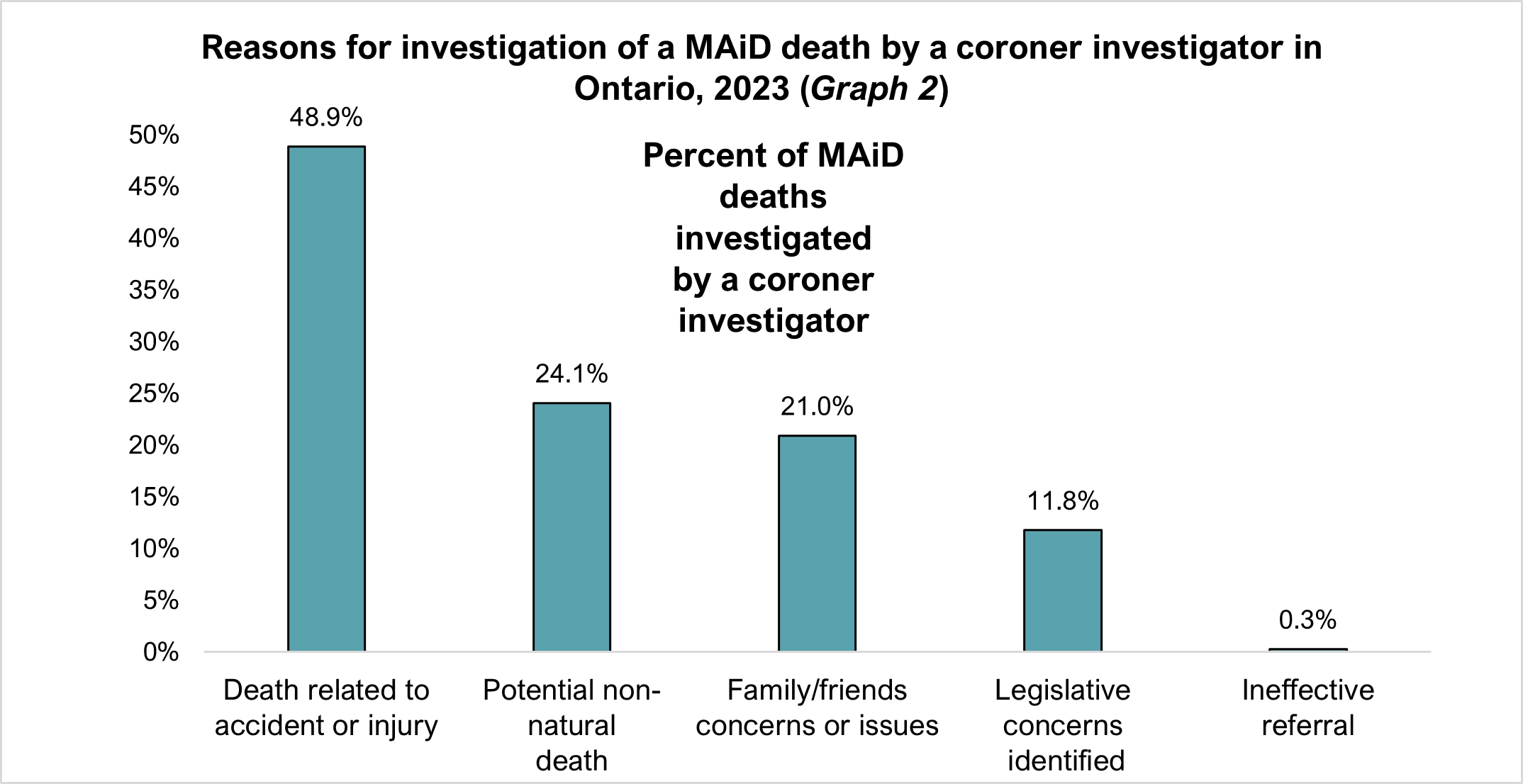
Note: multiple reasons may be selected for an investigation therefore totals do not add up to 100%
Practitioner data
In 2023, 70 new physicians and 8 new nurse practitioners (NPs) completed a MAiD provision. Since 2016, 775 individual physicians and 75 NPs have provided MAiD in Ontario. Of the 850 providers it is unknown how many physicians or NPs continue to provide MAiD. Most MAiD provisions were completed by physicians at 89% with NPs completing almost 11%. Further breakdown of MAiD provider statistics (both physicians and NPs combined) is found in Table 1: Track 1 Providers and Table 2: Track 2 Providers. In 2023, there were 460 individual providers for Track 1 and 62 individual providers for Track 2. Of the Track 2 providers, 59 were also Track 1 providers.
| Number of unique Track 1 providers | 460 |
|---|---|
| Percent of providers who performed ONE provision only | 23% |
| Percent of providers who performed 25% of all MAiD provisions | 2% |
| Average (and range of) provisions per provider | 9.8 (1-250) |
| Percent of providers performing MAiD in 4 or more public health units (PHUs) | 5% |
| Number of unique Track 2 providers | 62 |
|---|---|
| Percent of providers who performed ONE provision only | 66% |
| Percent of providers who performed 25% of all MAiD provisions | 5% |
| Average (and range of) provisions per provider | 1.8 (1-13) |
| Percent of providers performing MAiD in 4 or more public health units (PHUs) | 2% |
A breakdown of all MAiD providers and the number of Track 1 and Track 2 deaths by PHU is found in Table 3. This data demonstrates regional variations in MAiD provision rates based upon the number of available practitioners. MAiD providers will travel between PHUs with 5% of Track 1 providers (Table 1) and 2% of Track 2 providers (Table 2) doing provisions in 4 or more PHUs.
| PHU of MAiD patient | Total providers offering MAiD | Number of Track 1 cases | Track 1 cases per provider | Number of Track 2 cases | Track 2 cases per provider |
|---|---|---|---|---|---|
| Algoma Public Health | 4 | 42 | 10.5 | 1 | 1.0 |
| Brant County Health Unit | 11 | 57 | 5.2 | 0 | NA |
| Chatham-Kent Health Unit | 4 | 45 | 11.3 | 1 | 1.0 |
| City of Hamilton - Public Health & Social Services | 26 | 119 | 4.6 | 7 | 1.2 |
| Durham Region Health Department | 18 | 140 | 7.8 | 5 | 2.5 |
| Eastern Ontario Health Unit | 35 | 126 | 3.6 | 1 | 1.0 |
| Grey Bruce Health Unit | 31 | 160 | 5.2 | 2 | 1.0 |
| Haldimand-Norfolk Health Unit | 13 | 51 | 3.9 | 0 | NA |
| Haliburton, Kawartha, Pine Ridge District Health Unit | 31 | 149 | 4.8 | 4 | 1.0 |
| Halton Region Health Department | 25 | 214 | 8.6 | 8 | 2.7 |
| Hastings and Prince Edward Counties Health Unit | 20 | 75 | 3.8 | 1 | 1.0 |
| Huron Perth Health Unit | 18 | 126 | 7.0 | 3 | 1.5 |
| Kingston, Frontenac and Lennox & Addington Health Unit | 23 | 112 | 4.9 | 2 | 2.0 |
| Lambton Health Unit | 8 | 66 | 8.3 | 2 | 2.0 |
| Leeds, Grenville and Lanark District Health Unit | 38 | 137 | 3.9 | 3 | 1.0 |
| Middlesex-London Health Unit | 13 | 300 | 23.1 | 8 | 2.7 |
| Niagara Region Public Health Department | 10 | 145 | 16.1 | 4 | 1.3 |
| North Bay Parry Sound District Health Unit | 18 | 99 | 5.5 | 2 | 1.0 |
| Northwestern Health Unit | 18 | 38 | 2.2 | 1 | 1.0 |
| Ottawa Public Health | 37 | 318 | 8.8 | 5 | 2.5 |
| Peel Public Health | 28 | 162 | 6.0 | 2 | 1.0 |
| Peterborough County-City Health Unit | 15 | 83 | 5.5 | 2 | 1.0 |
| Porcupine Health Unit | 10 | 37 | 3.7 | 1 | 1.0 |
| Region of Waterloo Public Health | 17 | 106 | 6.2 | 2 | 1.0 |
| Renfrew County and District Health Unit | 13 | 57 | 4.4 | 0 | NA |
| Simcoe Muskoka District Health Unit | 54 | 258 | 5.1 | 15 | 1.2 |
| Southwestern Public Health | 13 | 153 | 11.8 | 3 | 3.0 |
| Sudbury and District Health Unit | 15 | 86 | 5.7 | 6 | 2.0 |
| Thunder Bay District Health Unit | 7 | 38 | 5.4 | 3 | 3.0 |
| Timiskaming Health Unit | 13 | 24 | 1.8 | 0 | NA |
| Toronto Public Health | 58 | 516 | 8.9 | 10 | 2.5 |
| Wellington-Dufferin-Guelph Health Unit | 24 | 128 | 5.6 | 4 | 1.0 |
| Windsor-Essex County Health Unit | 5 | 135 | 27.0 | 2 | 2.0 |
| York Region Public Health Services | 22 | 159 | 7.2 | 6 | 2.0 |
Note: Cases per provider are calculated based on the number of providers who provisioned MAiD of that Track.
In 2023, 47 Nurse Practitioners (NPs) completed 518 MAiD provisions (508 Track 1) MAiD provisions and 10 Track 2 provisions) or 11% of all provisions in Ontario.10 NPs provided 10 or more MAiD provisions, accounting for 391 provisions or 75% of all provisions completed by NPs.
Location of provision for NPs was 61% in the community and 39% within a hospital setting. This is a higher proportion of community provisions than seen with physicians, whose community provisions make up 47% of their MAiD provisions.
The involvement of NPs in MAiD work varies across the province due to organizational policies, compensation models or personal decisions as some NPs as part of their practice engage in both provisions and assessments while others provide only assessments or not at all. In deaths where the MAiD provider was a NP, the secondary assessor was a NP in 27% of deaths. When the MAiD provider was a physician, the secondary assessor was a NP in only 11% of deaths.
Further breakdown by PHU for NPs shows the distribution of NPs within the province who are engaged in MAiD work (Table 4). There are 6 PHUs with no NPs providing MAiD – particularly in eastern Ontario (Renfrew, Ottawa, and Eastern Ontario PHUs), while southwest Ontario has NPs providing a substantial number of provisions (Windsor, Essex, Lambton, and Chatham Kent PHUs). There are 7 PHUs where NPs have provided Track 2 provisions.
| PHU of MAiD patient | Number of nurse practitioners (NPs) providing MAiD | Number of Track 1 cases | Track 1 cases per NP | Number of Track 2 cases | Track 2 cases per NP |
|---|---|---|---|---|---|
| Algoma Public Health | 1 | 2 | 2.0 | 0 | NA |
| Brant County Health Unit | 1 | 1 | 1.0 | 0 | NA |
| Chatham-Kent Health Unit | 2 | 42 | 21.0 | 1 | 1.0 |
| City of Hamilton - Public Health & Social Services | 1 | 7 | 7.0 | 0 | NA |
| Durham Region Health Department | 2 | 6 | 3.0 | 0 | NA |
| Eastern Ontario Health Unit | 0 | NA | NA | NA | NA |
| Grey Bruce Health Unit | 3 | 8 | 2.7 | 0 | NA |
| Haldimand-Norfolk Health Unit | 3 | 4 | 1.3 | 0 | NA |
| Haliburton, Kawartha, Pine Ridge District Health Unit | 8 | 20 | 2.5 | 0 | NA |
| Halton Region Health Department | 1 | 1 | 1.0 | 0 | NA |
| Hastings and Prince Edward Counties Health Unit | 4 | 21 | 5.3 | 0 | NA |
| Huron Perth Health Unit | 2 | 4 | 2.0 | 0 | NA |
| Kingston, Frontenac and Lennox & Addington Health Unit | 1 | 4 | 4.0 | 0 | NA |
| Lambton Health Unit | 1 | 49 | 49.0 | 0 | NA |
| Leeds, Grenville and Lanark District Health Unit | 3 | 3 | 1.0 | 0 | NA |
| Middlesex-London Health Unit | 2 | 4 | 2.0 | 0 | NA |
| Niagara Region Public Health Department | 5 | 72 | 14.4 | 1 | 1.0 |
| North Bay Parry Sound District Health Unit | 1 | 1 | 1.0 | 0 | NA |
| Northwestern Health Unit | 1 | 1 | 1.0 | 0 | NA |
| Ottawa Public Health | 0 | NA | NA | NA | NA |
| Peel Public Health | 0 | NA | NA | NA | NA |
| Peterborough County-City Health Unit | 6 | 53 | 8.8 | 1 | 1.0 |
| Porcupine Health Unit | 2 | 4 | 2.0 | 1 | 1.0 |
| Region of Waterloo Public Health | 2 | 18 | 9.0 | 0 | NA |
| Renfrew County and District Health Unit | 0 | NA | NA | NA | NA |
| Simcoe Muskoka District Health Unit | 5 | 12 | 4.0 | 3 | 1.0 |
| Southwestern Public Health | 0 | 0 | 0.0 | 0 | NA |
| Sudbury and District Health Unit | 2 | 9 | 4.5 | 1 | 1.0 |
| Thunder Bay District Health Unit | 0 | NA | NA | NA | NA |
| Timiskaming Health Unit | 1 | 1 | 1.0 | 0 | NA |
| Toronto Public Health | 1 | 3 | 3.0 | 0 | NA |
| Wellington-Dufferin-Guelph Health Unit | 2 | 6 | 3.0 | 0 | NA |
| Windsor-Essex County Health Unit | 3 | 132 | 44.0 | 2 | 2.0 |
| York Region Public Health Services | 2 | 14 | 7.0 | 0 | NA |
Note: Cases per NP are calculated based on the number of NPs who provisioned MAiD of that Track
Practitioner feedback
As part of the oversight process, the OCC has established a leveled feedback response to any legislative or practice issues identified following review or investigation of a death. Level 1 and Level 2 responses are intended to offer resources and guidance for noted practice or legislative issues. In 2023, the overall response rate was 4%, with 3.7% of the responses for Track 1 provisions and 14.7% of responses for Track 2. The MRT followed up with informal conversations most frequently (Level 1 response) upon completion of an investigation (Graph 3).
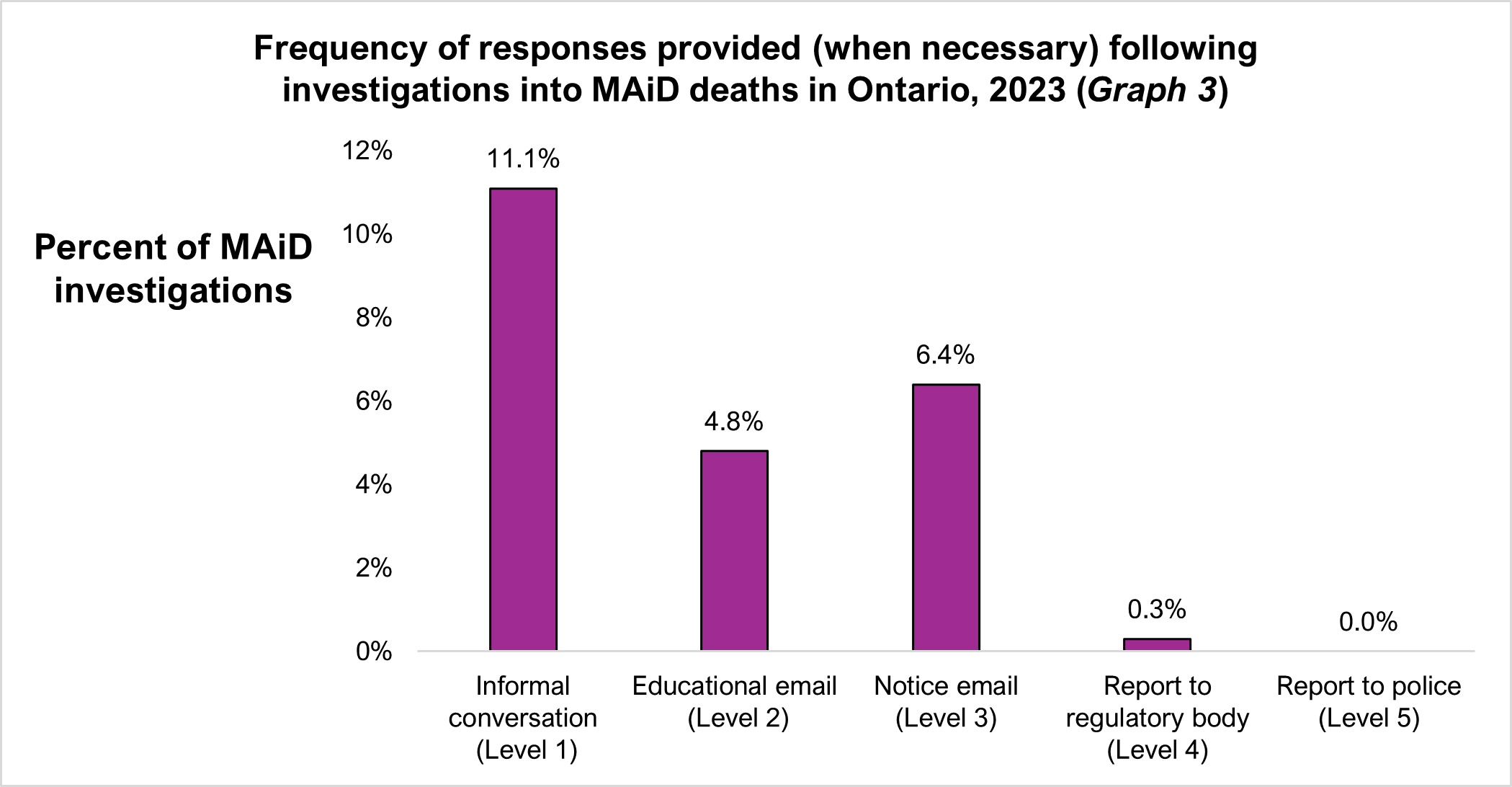
In 6% of 2023 MAiD deaths level 3 email notices were issued when specific legislative concerns were identified or unmet following review. Report to the regulatory body for the practitioner (College of Physicians and Surgeons of Ontario or the College of Nurses of Ontario) is uncommon and occurs in the event of significant practice deviation or repeated level notice from the OCC. To date, there has been no Level 5 response in Ontario. For more information regarding the level response framework please refer to the Medical assistance in dying memorandum.
Recommendations
As part of its mandate, the MAiD Review Team (MRT) seeks to promote safe MAiD practice through knowledge translation based on the learnings obtained from the MAiD death review process. This knowledge is shared with a variety of stakeholders: Ministries of government (provincial and federal), advocacy groups, organizations, MAiD practitioners, regulatory colleges, amongst others.
Members of the MRT, with input from experts in various fields, have contributed to the development and dissemination of various topics to improve access to MAiD, support practice enhancement and inform policy. Some of the topics and communications developed and shared by the OCC include:
- Intraosseous administration of MAiD
- Safe Handling of MAiD Medications Kits
- Private Pay Nursing Services for Intravenous Access in the Community
- Voluntariness Considerations for Joint MAiD Provisions
- Track 2 (Non-RFND) Legislative and Safeguards Concerns: Lessons Learned
The MRT continues to identify aspects of MAiD practice that require further evaluation and analysis. In conjunction with the newly formed MAiD Death Review Committee (MDR) and greater access to expertise in areas of law, medicine, and ethics, the MRT expects to expand on these topics with guidance for those involved with MAiD at the clinical and policy levels with a goal to help inform and shape MAiD practice in Ontario.
Ontario data and trends
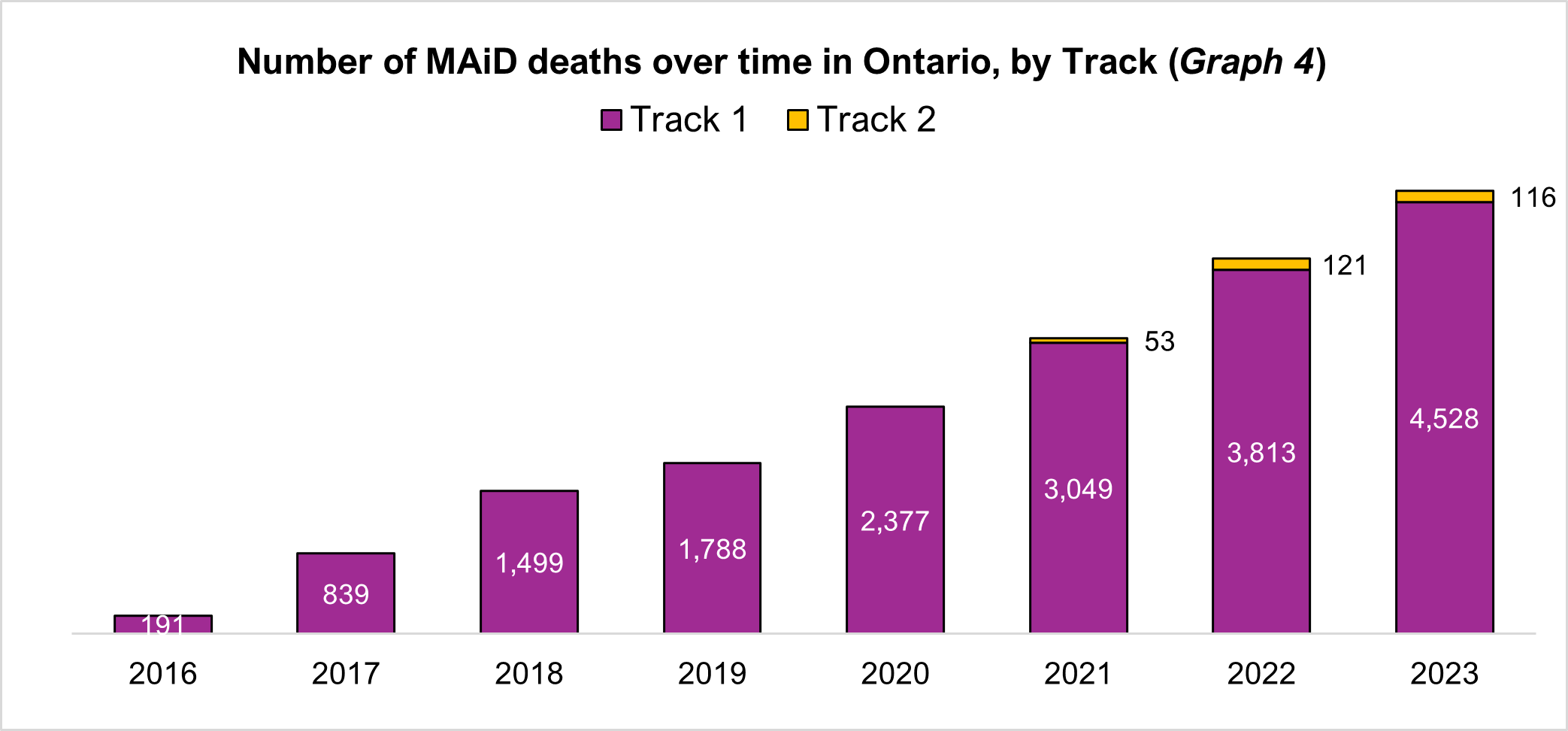
MAiD deaths in Ontario over time
There have been 18,374 MAiD deaths in Ontario since 2016 showing an increase of 454% since 2017. Since 2021 with the change in legislation with Bill C-7, Track 1 deaths have increased by 49% and Track 2 deaths, despite a small decline in 2023, have increased by 119%. In 2023, Track 2 MAiD deaths made up 2.4% of all MAiD deaths.
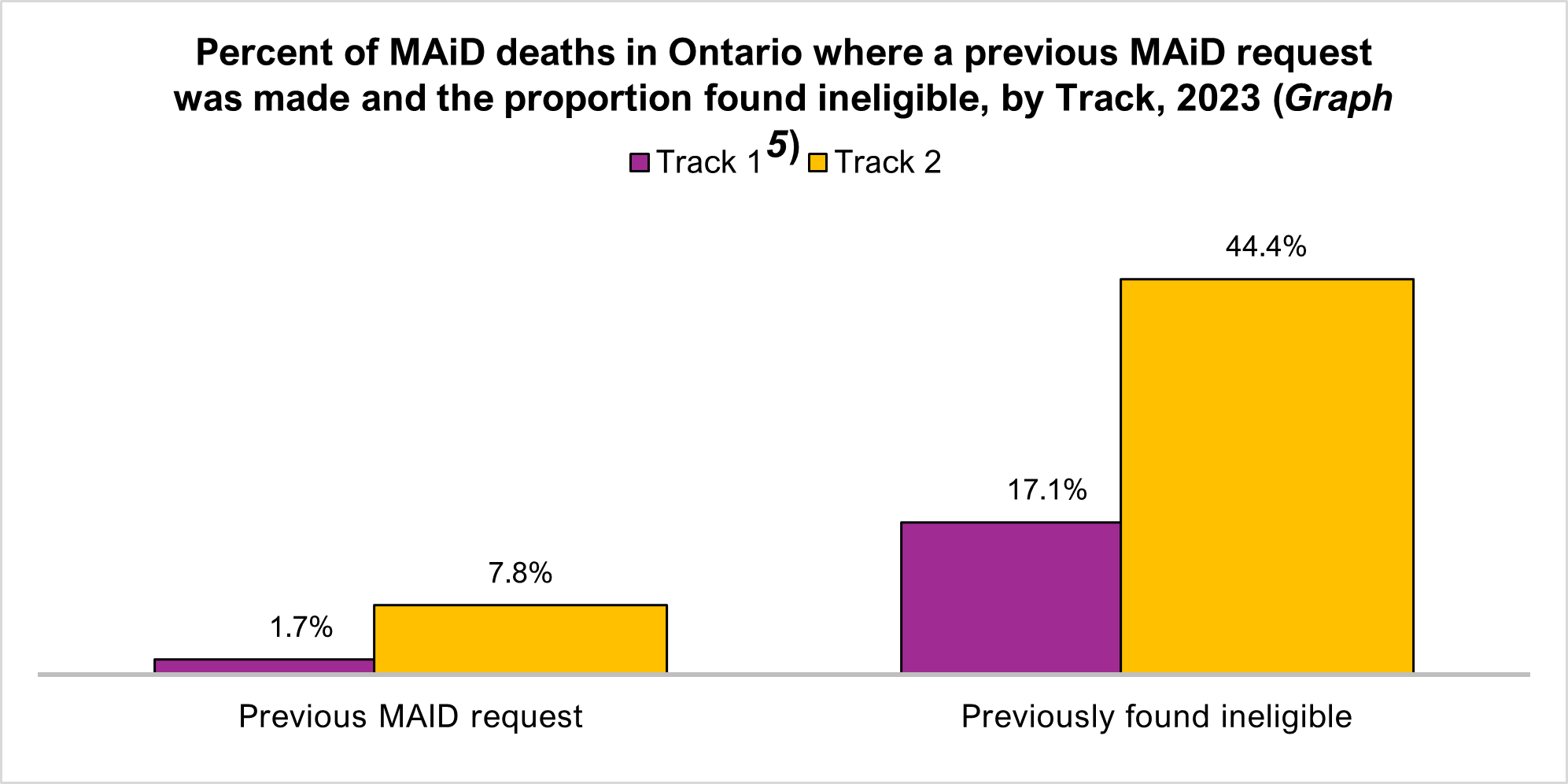
Previous MAiD requests
Information on prior requests for MAiD was captured and reasons why MAiD did not proceed included a finding of ineligibility, withdrawal of the request, request not actioned, or duration of time between finding of eligibility and assessment. Nearly 8% of Track 2 cases had a previous request for MAiD versus 2% for Track 1. 44% of Track 2 cases in Ontario were found ineligible for previous MAiD requests in contrast to 17% for Track 1 requests.
At times requests for MAiD are made urgently resulting in a short duration of time between the two assessments for eligibility and the provision of MAiD. In 2023, 54 requests for same day assessments and provision were reported (less than 24 hours), and 154 provisions occurred the day after a request (within 24 hours).
Transfer for provision
Since 2023 Health Canada reporting requirements includes the need for transfer for MAiD provision which can occur for many reasons. In Ontario, 8% of MAiD provisions required a transfer as reported by the MAiD practitioner on the MDR. The most common reason for transfer for MAiD was due to a patient request (49% of all patient transfers) followed by organizational policies (44%) which was usually due to MAiD not being permitted within the organization.
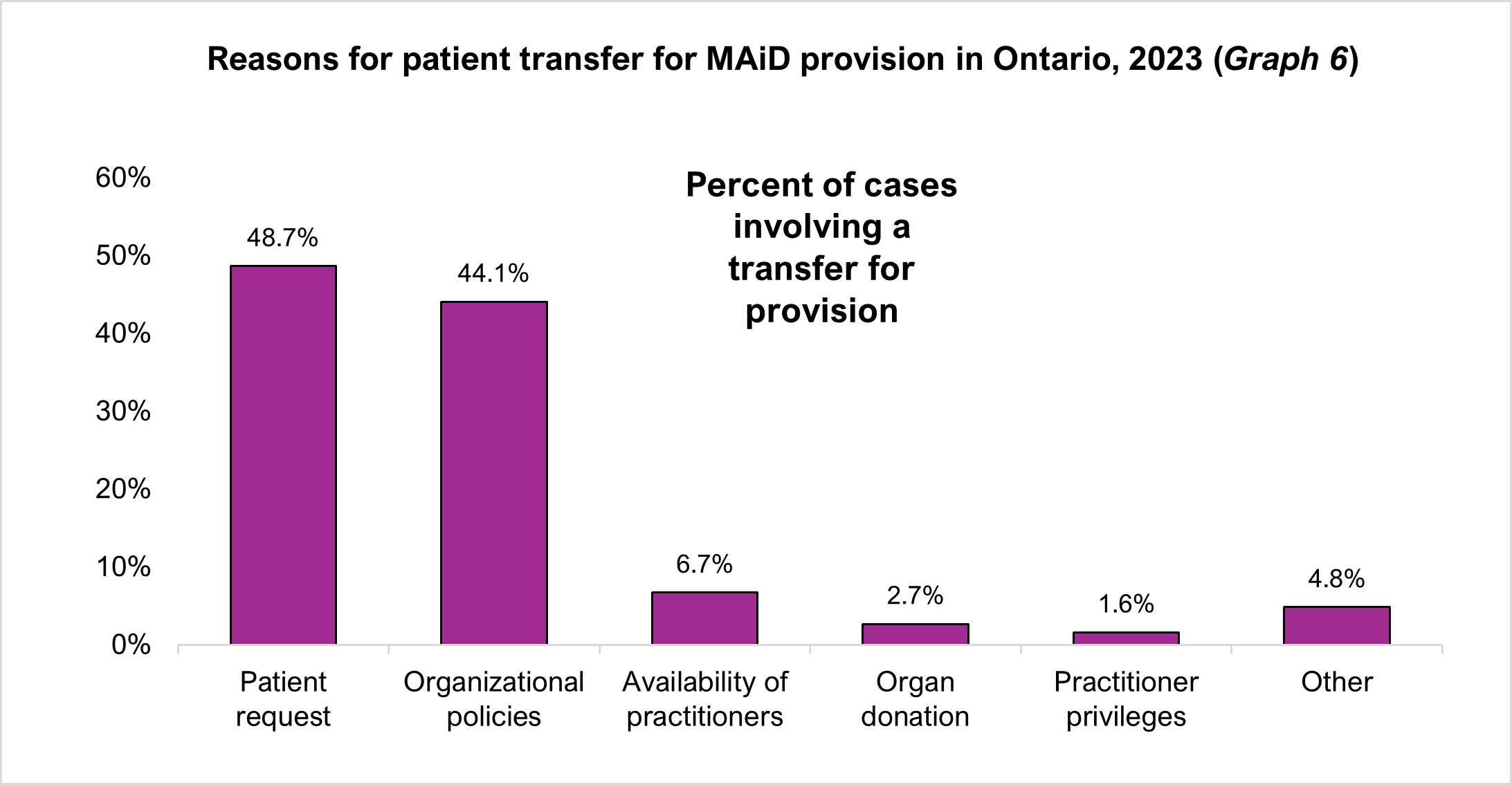
Note: multiple reasons may be selected for a transfer therefore totals do not add up to 100%
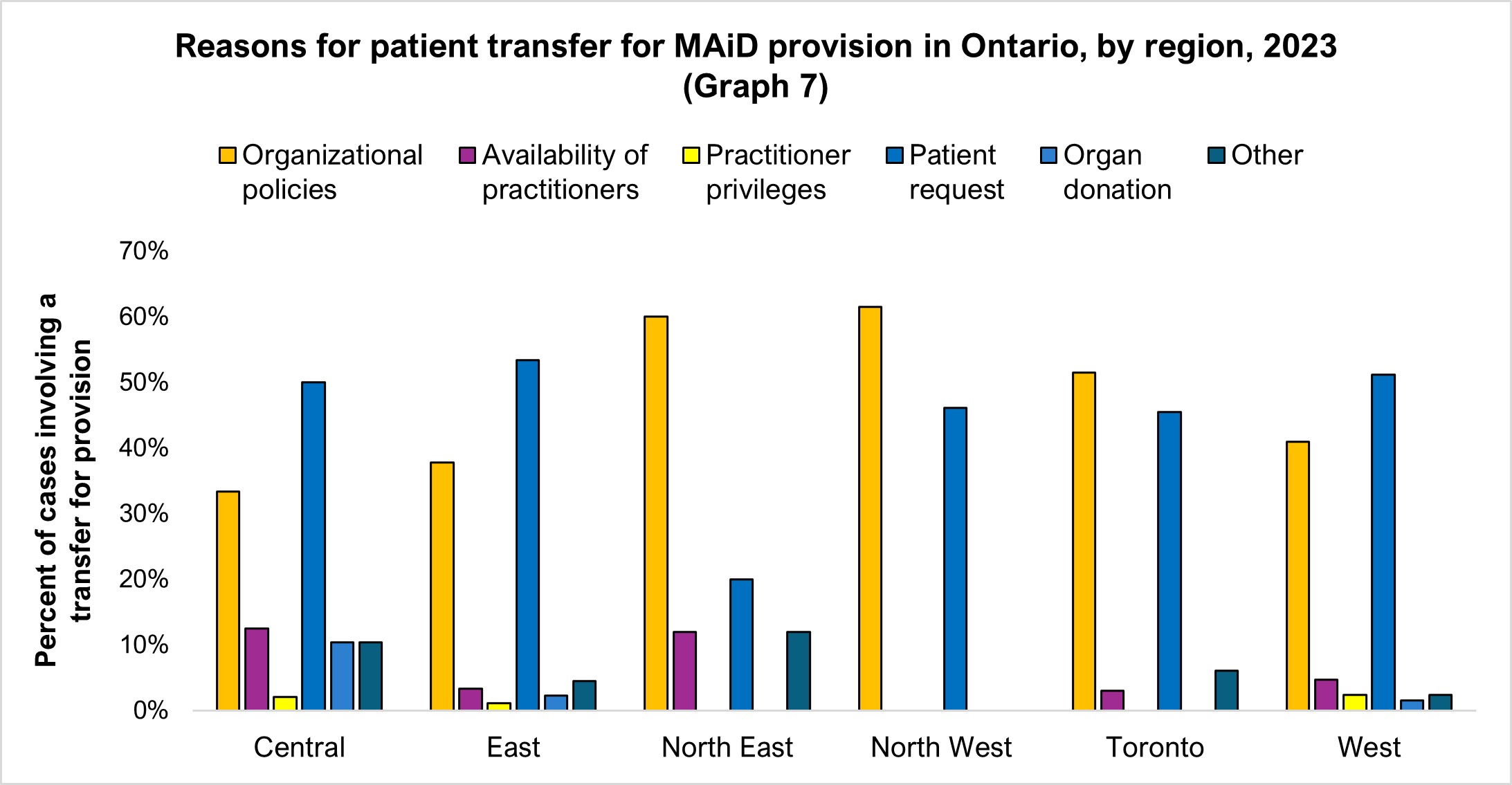
Further breakdown within the province as to where the transfers most frequently occur shows the North West and North East regions with the highest number of transfers due to organizational policies with transfers based on patient request higher in the East and Central regions of the province. Transfers for organ donation were highest in the Central region.
Complications reported
The MDR allows MAiD providers to share any complications encountered before, during or after the MAiD provision. In 2023 this information was provided in 82 deaths (1.8%). The most common complication reported was challenges with intravenous (IV) initiation or poor IV access which occurred in 53.7% of the complications reported. The IV line going interstitial (outside of the vein) was the second most common complication encountered at 31.7%.
| Type of complication | Percent of MAiD deaths with complications |
|---|---|
| Poor intravenous (IV) initiation or access | 53.7% |
| IV line interstitial | 31.7% |
| Further dosage required | 6.1% |
| Unexpected medication effects | 3.7% |
| Location/setting | 1.2% |
| Equipment malfunction | 1.2% |
| Family disagreement at time of MAiD provision | 1.2% |
| Existing patient condition | 1.2% |
Next of kin: Track 1 vs. Track 2
Following every reported MAiD death in Ontario, a next of kin representative of the deceased person is contacted. During the conversation opportunity is provided to identify concerns or issues that may have been encountered either prior to or during the MAiD process. The majority of these conversations take place with a child of the deceased person with a higher number of Track 2 provisions involving friends or other relationships.
Next of Kin: Concerns raised
Of the 83 reports shared with the MRT in 2023, most of the concerns were related to the MAiD process or provision at 58% (Graph 9). Specific concerns involved the application process (ineffective referral, lack of information, delays in assessments), and perceived lack of communication (regarding the procedure, medications, unexpected reactions).
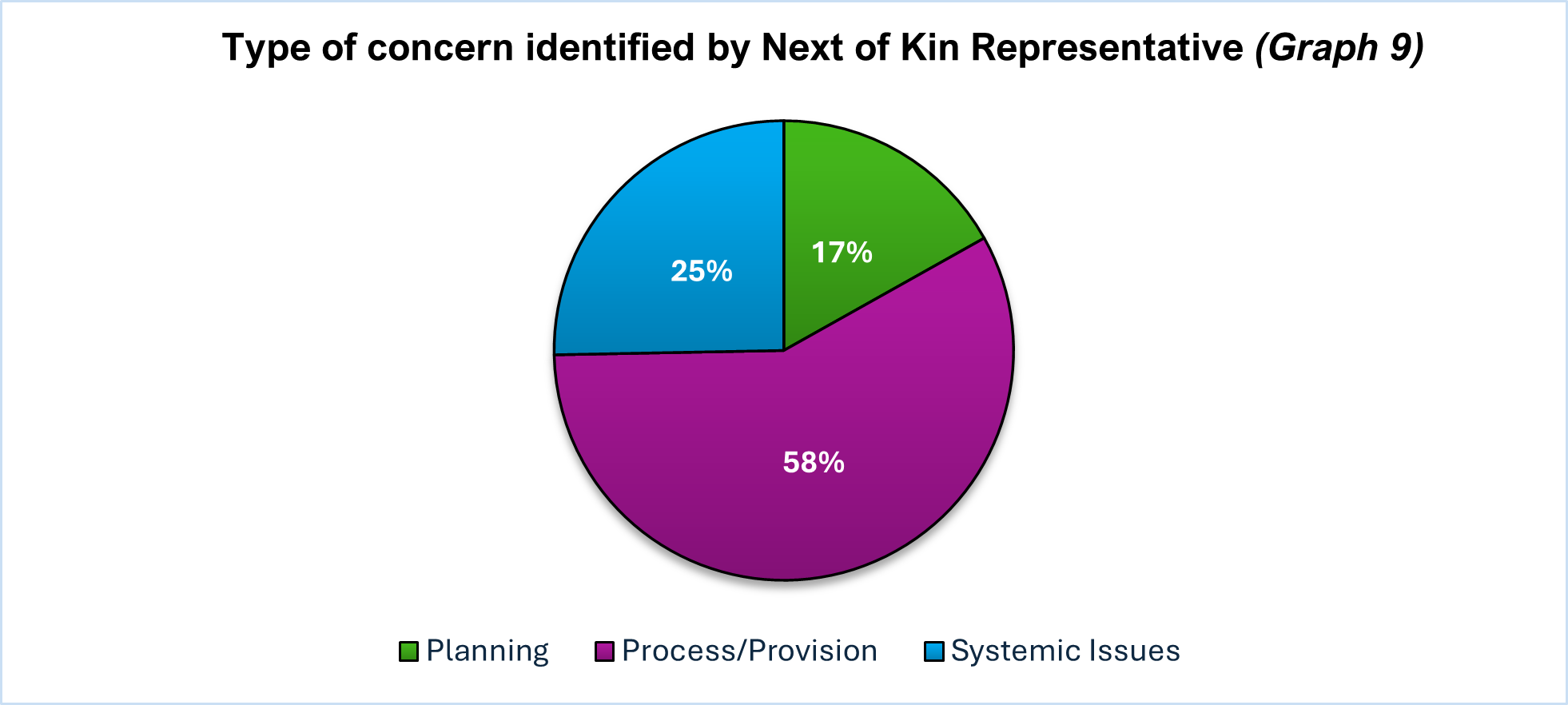
Systemic issues (25%) identified by NOK representatives focused on timely access to providers and assessors, availability of nursing, paying for private nursing for IV insertions and access to facilities that participate in MAiD.
Planning concerns (17%) were often connected to issues arising from challenges faced in the planning of MAiD and the time period leading up to the MAiD provision and included the care received in the institution, care approach of care providers, access to health care services and treatments (alternatives offered to MAiD). Additional issues identified were related to professionalism, where the provision would occur, health care provider schedules that interfered with provisions, and miscommunication about what was to happen following the provision.
The MRT has different methods to address these concerns, including feedback to the MAiD practitioner, guidance to the NOK on who to contact to explore care-related concerns, communication with organizations regarding policies and practices, and sharing of findings with Ministry of Health where access concerns arise. Most concerns raised by NOK representatives were resolved during the initial phone call (58 of 83) with no further action felt to be necessary.
Capturing the wide variety of concerns and issues identified by the NOK representative is an evolving area of data collection for the MRT. It is important to understand and document the experiences of those who have chosen to access an assisted death as told through their loved ones.
Conclusion
The modernization of MAiD reporting in Ontario has provided opportunities for enhanced data collection and analysis helping gain greater insight into MAiD practice in addition to the individuals who request an assisted death and those providing this service. This initial report on the oversight model and review processes of the MAiD Review Team (MRT) situated within the Office of the Chief Coroner is intended to increase transparency and inform stakeholders of the efforts and commitment to ensuring that every MAiD death is provided according to the Criminal Code and in the most compassionate and dignified manner. The MRT believes that opportunities to influence and support MAiD practice identified during the review process will benefit practitioners and the people of Ontario.
Thank you
The data presented in this report would not have been possible without the support of the Death Analytics, Safety and Health Unit at the Office of the Chief Coroner. The ability to transform the information collected during the review process into relational and meaningful information is greatly appreciated.
This data is only as good as the practitioners who provide it as part of their reporting obligations, and we recognize and are grateful for the time and detail that goes into the reporting of every MAiD death.
Finally, the contributions of the MRT, who spend every day speaking with loved ones, reviewing records and ensuring that the narrative of the lives of those who have sought an assisted death are represented accurately and with great care cannot be overstated and is greatly valued.